
Musculoskeletal Radiology — MCQs

On this page
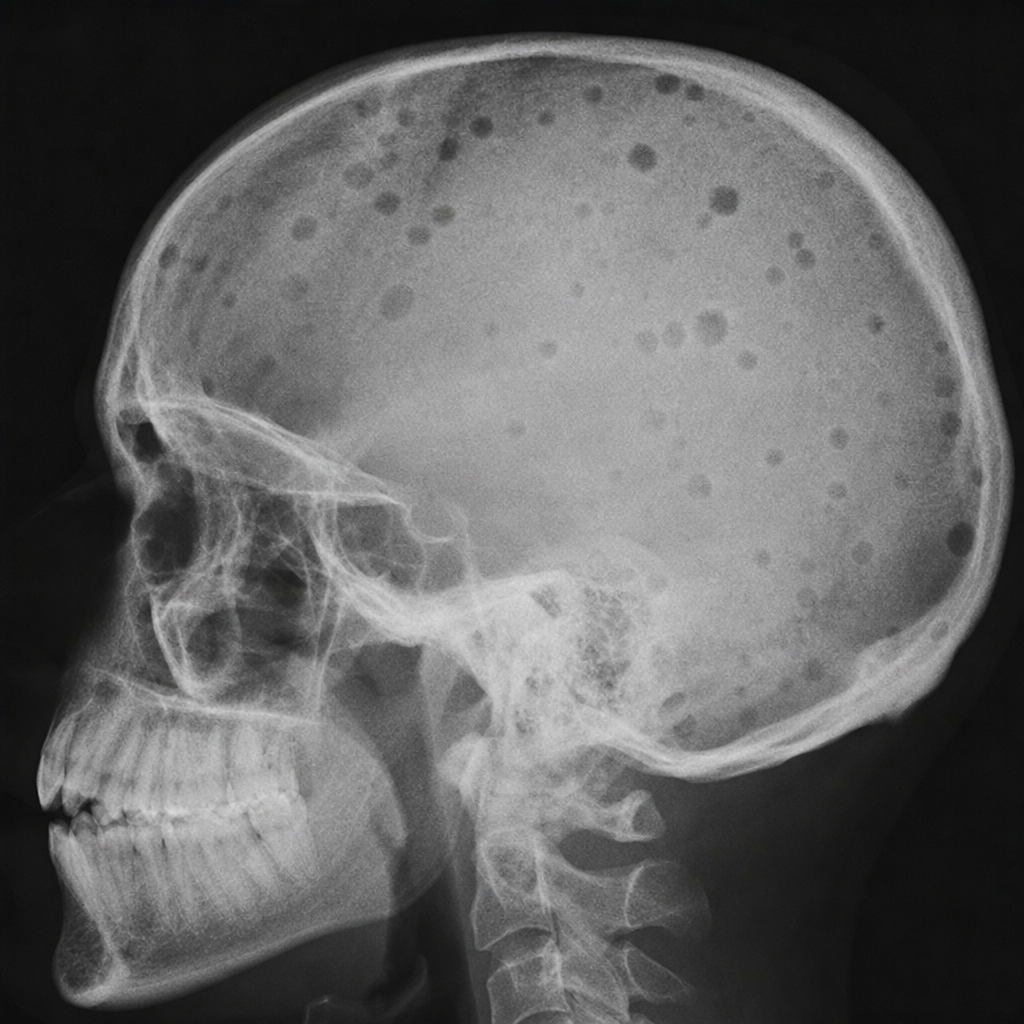
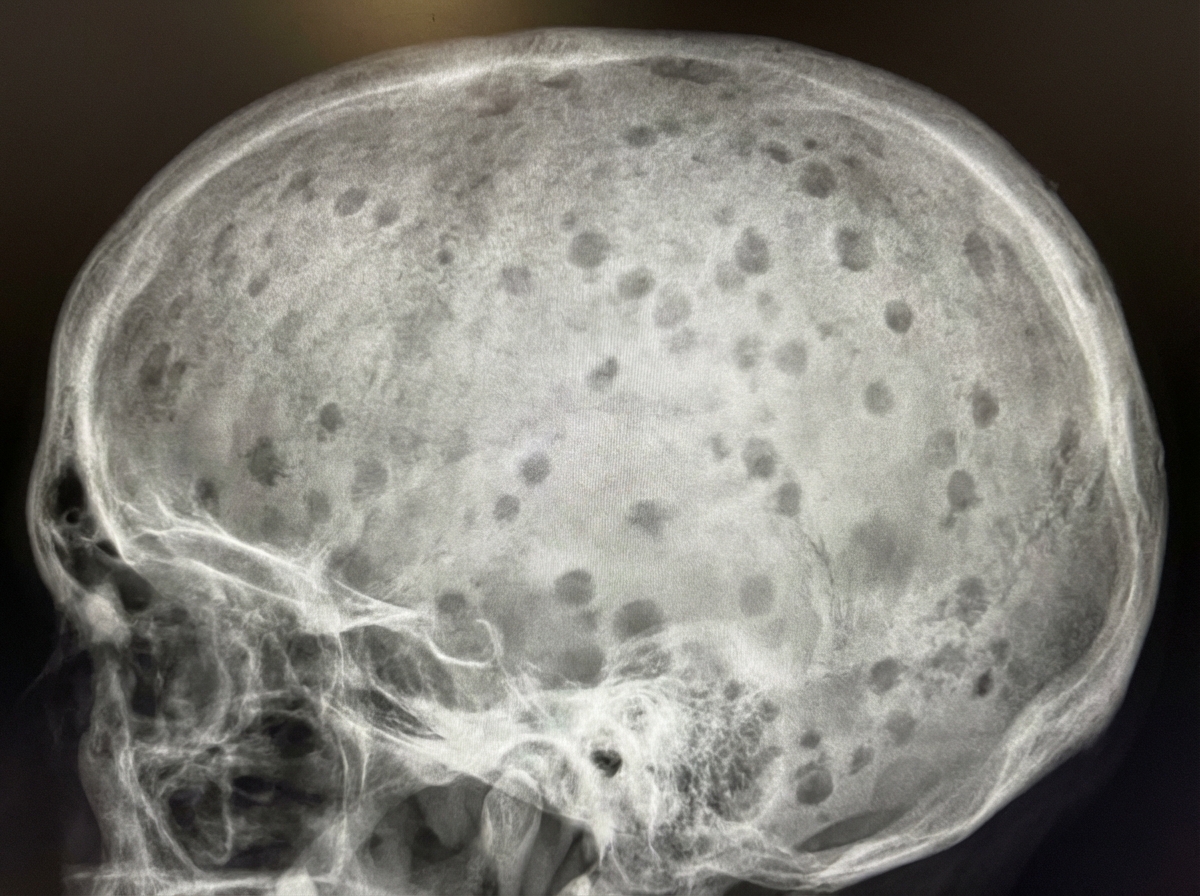
A 60-year-old man presents with bone pain and fatigue. His skull X-ray is shown in the image. This appearance is most suggestive of which of the following conditions?
On X-ray, joint swelling and intra-articular calcification appearance is seen in which condition?
Ankylosis of the temporomandibular joint (TMJ) can be best visualized in which radiographic view?
Which of the following is NOT a radiological feature of scleroderma?
X-ray skull characteristically shows "Hair on end" appearance in which of the following diseases?
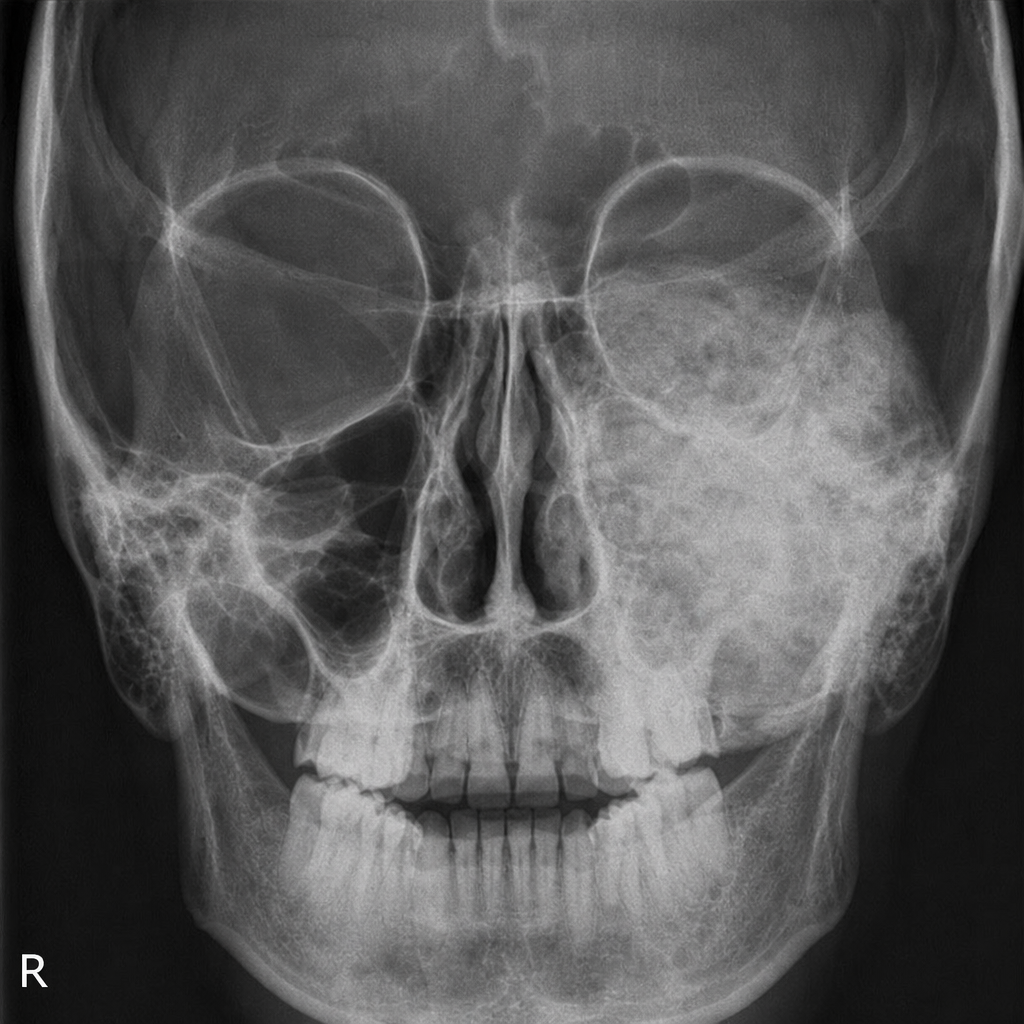
What is shown in the X-ray skull?
The "Double PCL" sign on MRI knee is typically seen in which of the following conditions?
Which is the earliest radiologic feature of bone infection?
The radiographic finding of the left maxilla indicates which of the following?
An 'H' shaped vertebra is characteristic of which condition?
Practice by Chapter
Radiographic Anatomy of Bones and Joints
Practice Questions
Imaging of Fractures and Dislocations
Practice Questions
Arthritides: Inflammatory and Degenerative
Practice Questions
Metabolic Bone Diseases
Practice Questions
Bone and Soft Tissue Tumors
Practice Questions
Congenital Skeletal Anomalies
Practice Questions
Spine Imaging
Practice Questions
Skeletal Infections
Practice Questions
Sports Medicine Imaging
Practice Questions
Imaging of Prostheses and Implants
Practice Questions
Musculoskeletal Ultrasound
Practice Questions
MSK Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app