
Musculoskeletal Radiology — MCQs

On this page
In Scurvy, Wimberger's sign is best seen in which location?
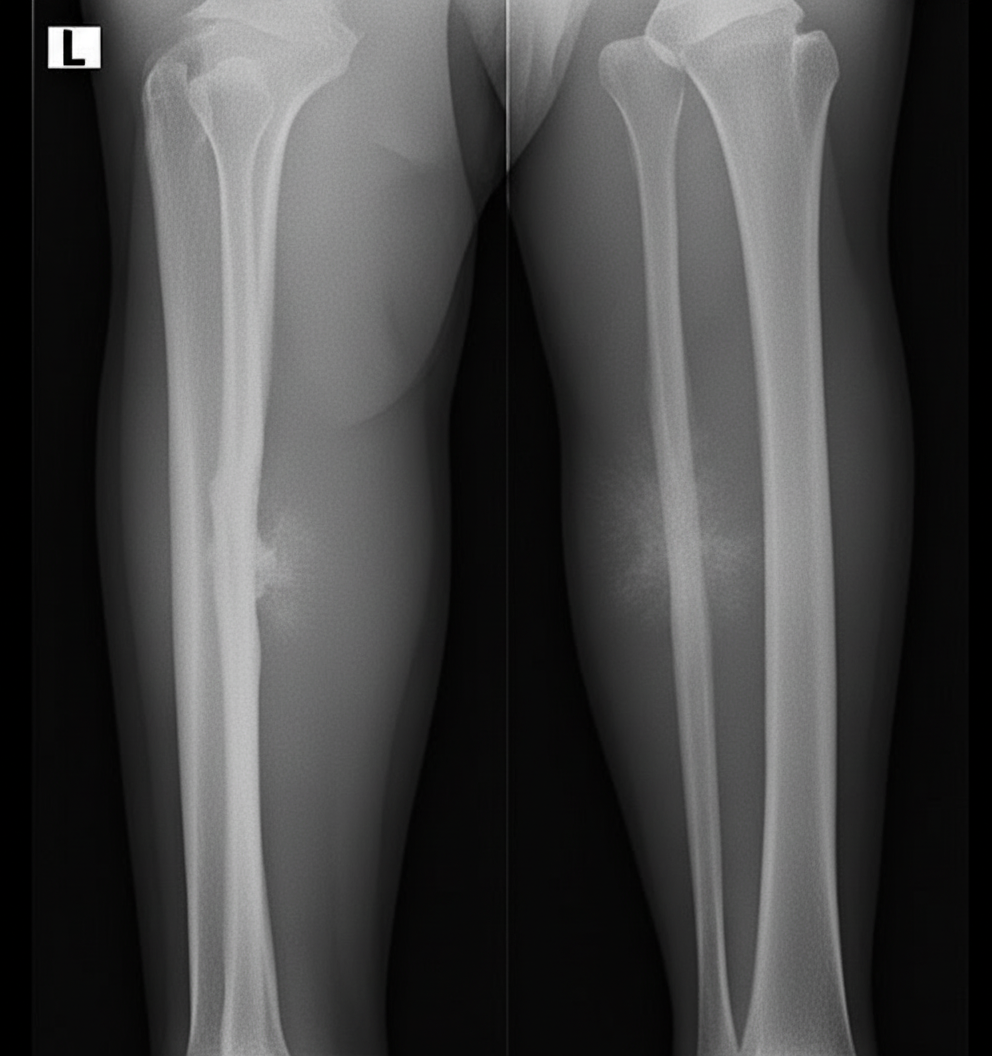
An X-ray of the right proximal tibia and fibula is shown. What condition does it possibly represent?
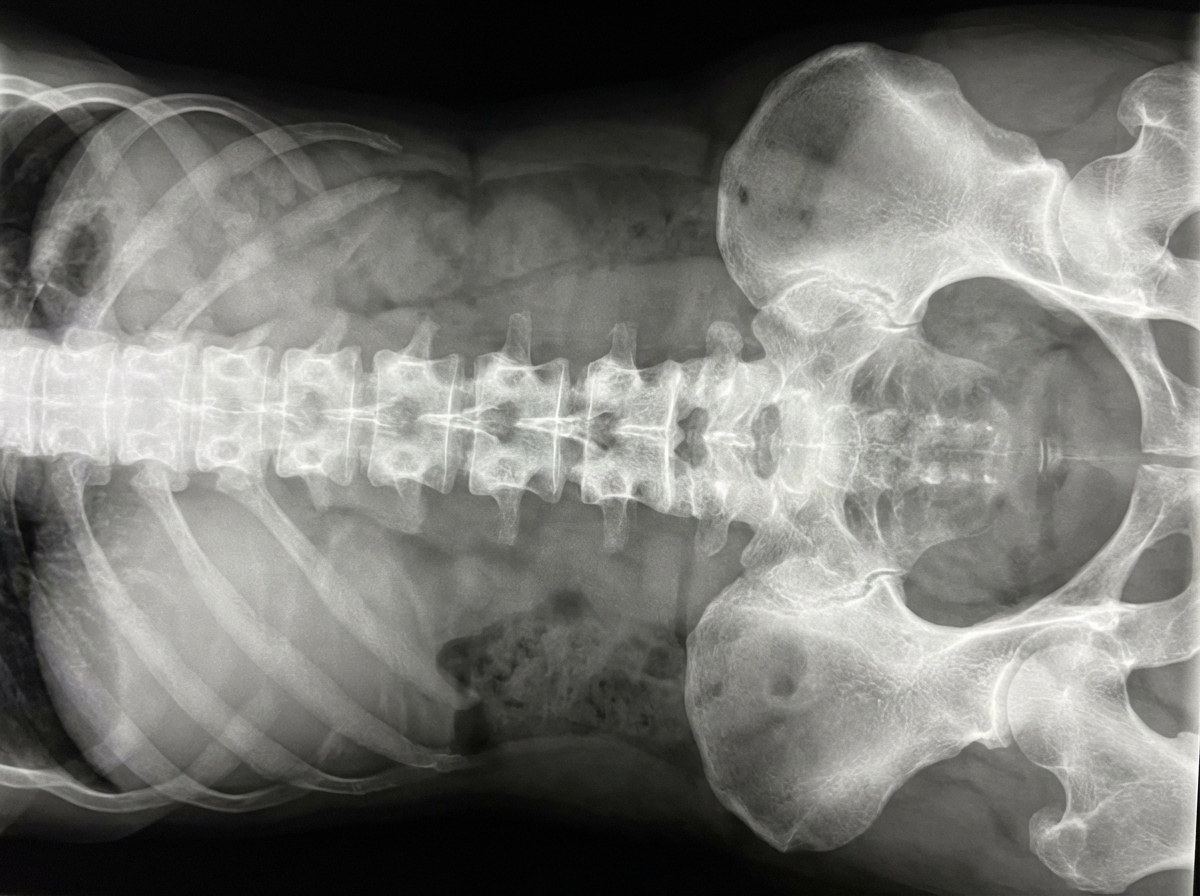
Which of the following is the most probable diagnosis given the provided X-ray?
The "salt and pepper" appearance of the skull is typically seen in which of the following conditions?
The 'Pelkan spur' is a radiological feature of which of the following conditions?
Tufting of the distal phalanx is characteristically seen in which condition?
Bullet shaped vertebrae are seen in all of the following conditions, EXCEPT:
Stippled epiphysis is seen in which condition?
Disk perforation is best examined by?
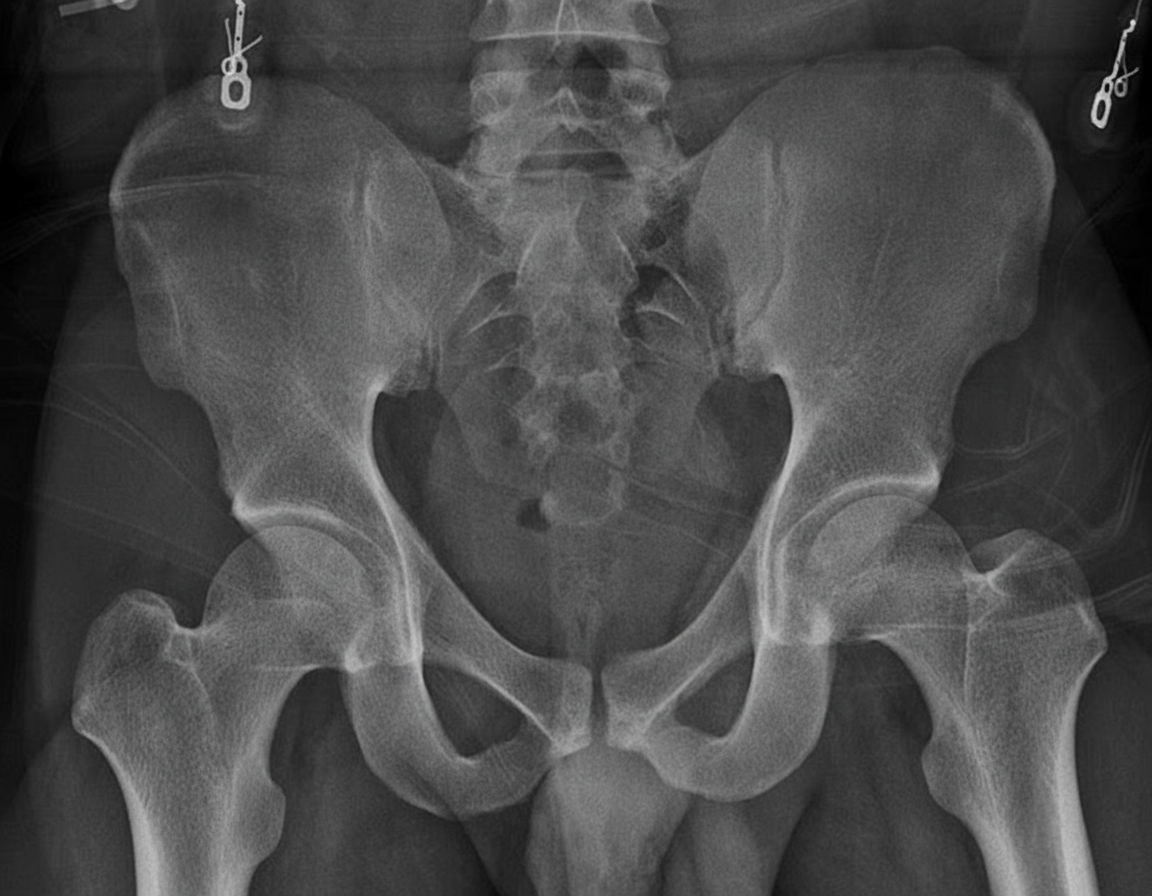
The following Pelvic Radiograph is seen in which condition?
Practice by Chapter
Radiographic Anatomy of Bones and Joints
Practice Questions
Imaging of Fractures and Dislocations
Practice Questions
Arthritides: Inflammatory and Degenerative
Practice Questions
Metabolic Bone Diseases
Practice Questions
Bone and Soft Tissue Tumors
Practice Questions
Congenital Skeletal Anomalies
Practice Questions
Spine Imaging
Practice Questions
Skeletal Infections
Practice Questions
Sports Medicine Imaging
Practice Questions
Imaging of Prostheses and Implants
Practice Questions
Musculoskeletal Ultrasound
Practice Questions
MSK Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app