
Musculoskeletal Radiology — MCQs

On this page
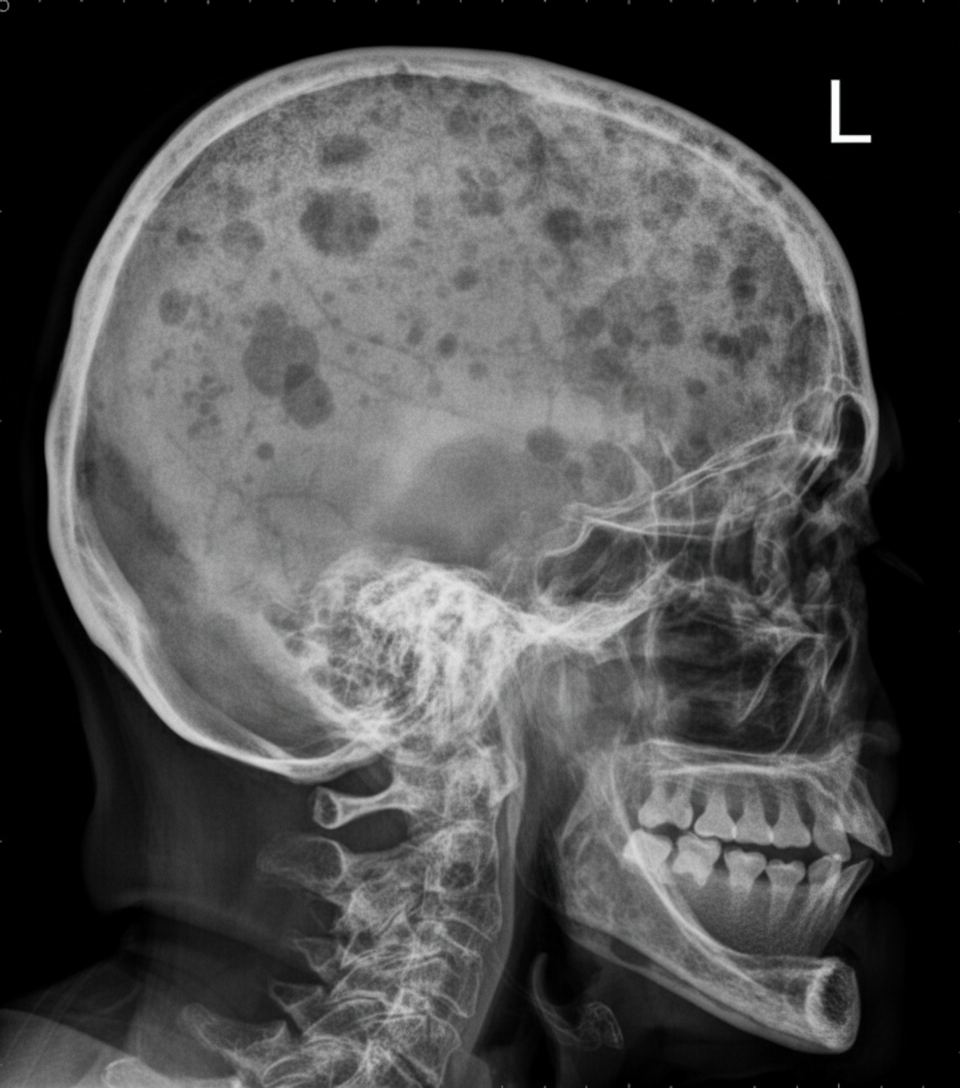
The lateral skull radiograph shows numerous well-circumscribed, punched-out lytic lesions. Which condition is most strongly associated with this finding?
A 48-year-old man with a long history of low back pain presents with similar symptoms. His previous X-ray 6 years ago showed degenerative disc changes. What should be done next?
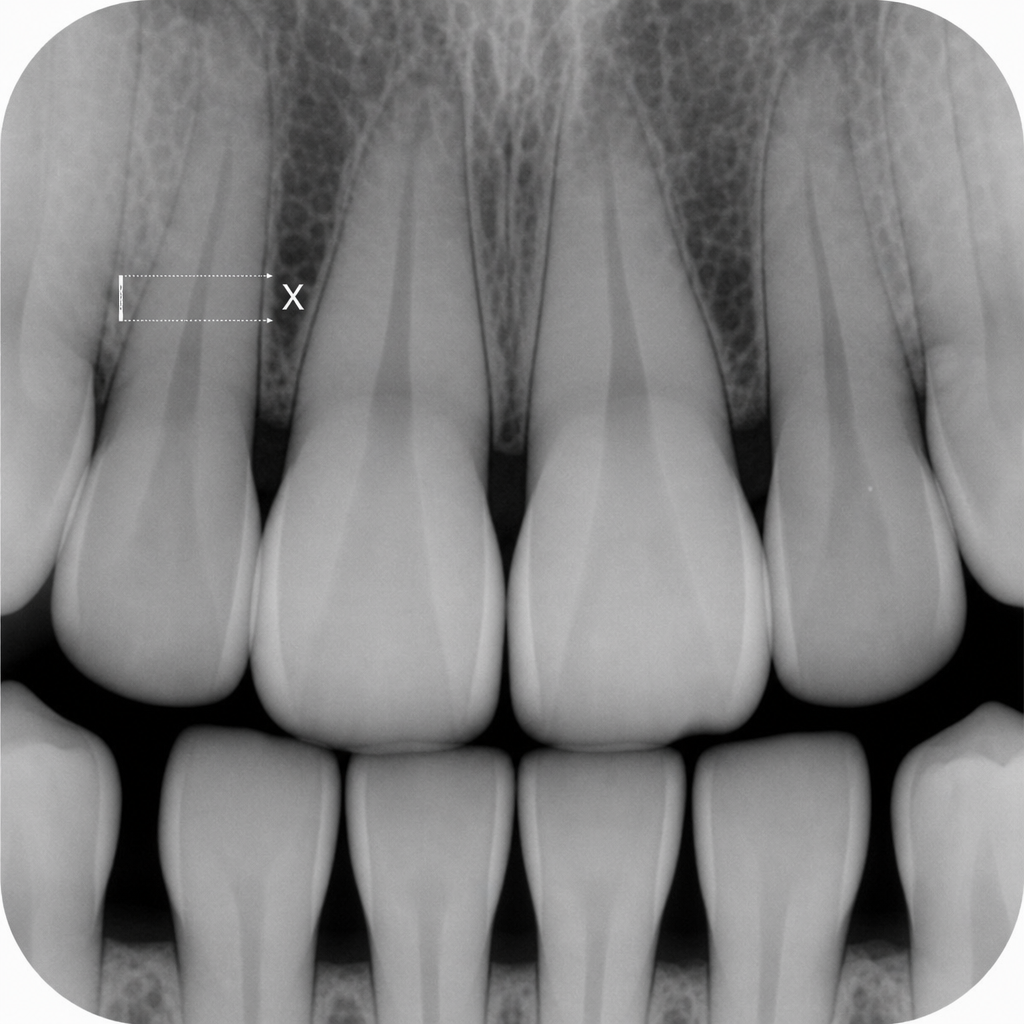
In the following radiograph, X represents the measured distance from the cementoenamel junction (CEJ) to the alveolar crest. Which of the following best represents the bone loss?
Which of the following is NOT a radiological feature of scleroderma?
Which of the following conditions is NOT associated with the 'bone within a bone' appearance?
In ankylosing spondylitis, what are the first radiological changes seen?
Which of the following is not a type I geographic lesion of bone?
What is the earliest radiological sign indicative of sacroiliitis on X-ray?
Shenton's line is a radiological line used to determine the pathology of:
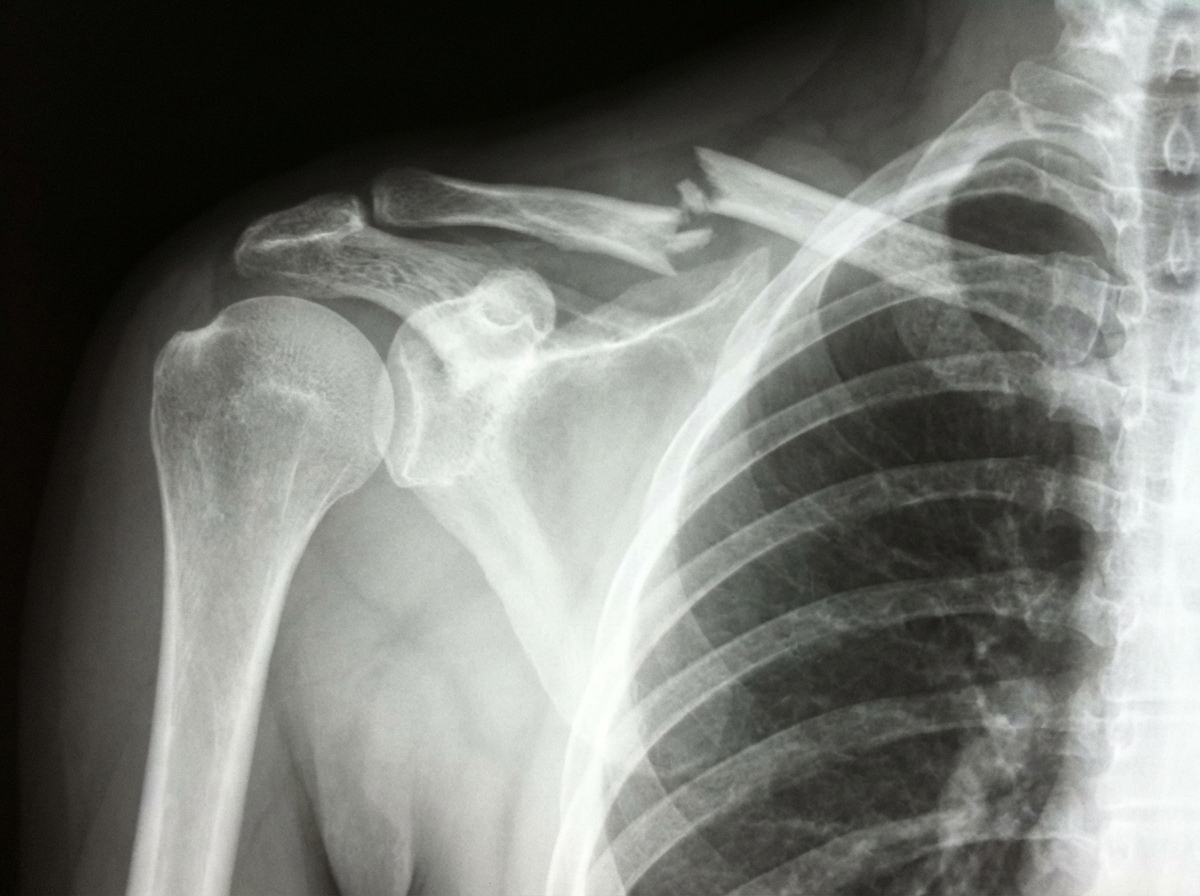
What is the finding seen on X-ray of the right shoulder?
Practice by Chapter
Radiographic Anatomy of Bones and Joints
Practice Questions
Imaging of Fractures and Dislocations
Practice Questions
Arthritides: Inflammatory and Degenerative
Practice Questions
Metabolic Bone Diseases
Practice Questions
Bone and Soft Tissue Tumors
Practice Questions
Congenital Skeletal Anomalies
Practice Questions
Spine Imaging
Practice Questions
Skeletal Infections
Practice Questions
Sports Medicine Imaging
Practice Questions
Imaging of Prostheses and Implants
Practice Questions
Musculoskeletal Ultrasound
Practice Questions
MSK Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app