
Musculoskeletal Radiology — MCQs

On this page
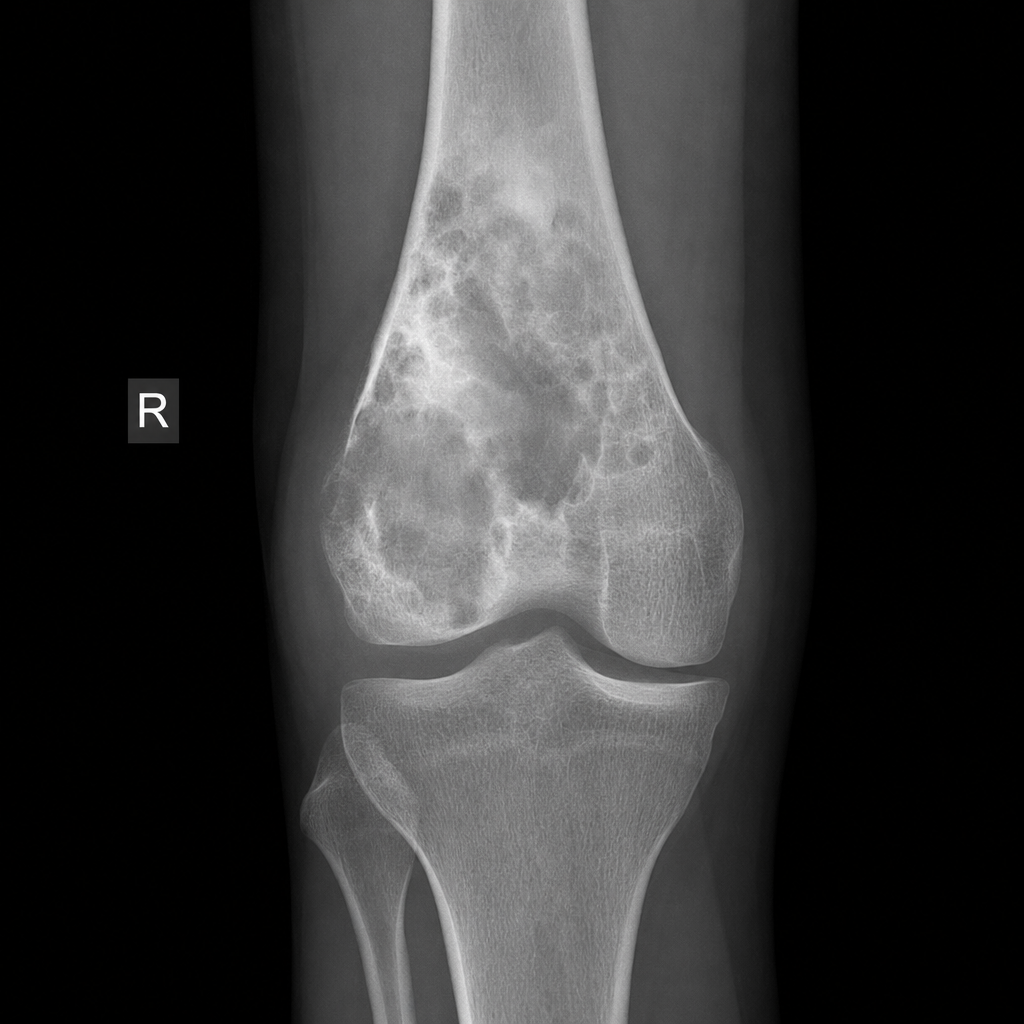
A 16-year-old male presents with a 6-week history of progressively worsening pain and swelling around the right knee. The pain is worse at night and does not respond to analgesics. There is no history of trauma. Serum alkaline phosphatase is markedly elevated. A plain radiograph of the distal femur is shown in Image 3. Which investigation should be performed next to best assess local extent of disease and guide surgical planning?
Superior rib notching is caused by which of the following?
What is the most common source of error leading to a false positive finding of dental caries?
Spoke wheel calcification in an osteolytic lesion is seen in which of the following conditions?
A radiolucency in bone without periosteal bone reaction is seen in which of the following conditions?
Practice by Chapter
Radiographic Anatomy of Bones and Joints
Practice Questions
Imaging of Fractures and Dislocations
Practice Questions
Arthritides: Inflammatory and Degenerative
Practice Questions
Metabolic Bone Diseases
Practice Questions
Bone and Soft Tissue Tumors
Practice Questions
Congenital Skeletal Anomalies
Practice Questions
Spine Imaging
Practice Questions
Skeletal Infections
Practice Questions
Sports Medicine Imaging
Practice Questions
Imaging of Prostheses and Implants
Practice Questions
Musculoskeletal Ultrasound
Practice Questions
MSK Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app