
Emergency Radiology — MCQs

On this page
What is the investigation of choice for the evaluation of acute head injury?
Which radiographic view is best for detecting hollow viscus perforation?
The X-ray image provided (img-41.jpeg) shows multiple cylindrical objects in the abdominal area. Which of the following conditions is most likely represented by this image?
A 30 year old apparently healthy man who was carrying laxatives and enema apparatus developed abdominal pain at the airport and an x-ray was done which appears as shown below. Which of the following is the likely diagnosis?
Following a fight between 2 groups, a boy was brought with severe pain in the chest, distended neck veins, dyspnea, and a BP of 80/50 mmHg. X-ray shows the following findings: What is the diagnosis?
Whole-body CT scan protocol for a trauma patient includes all, except
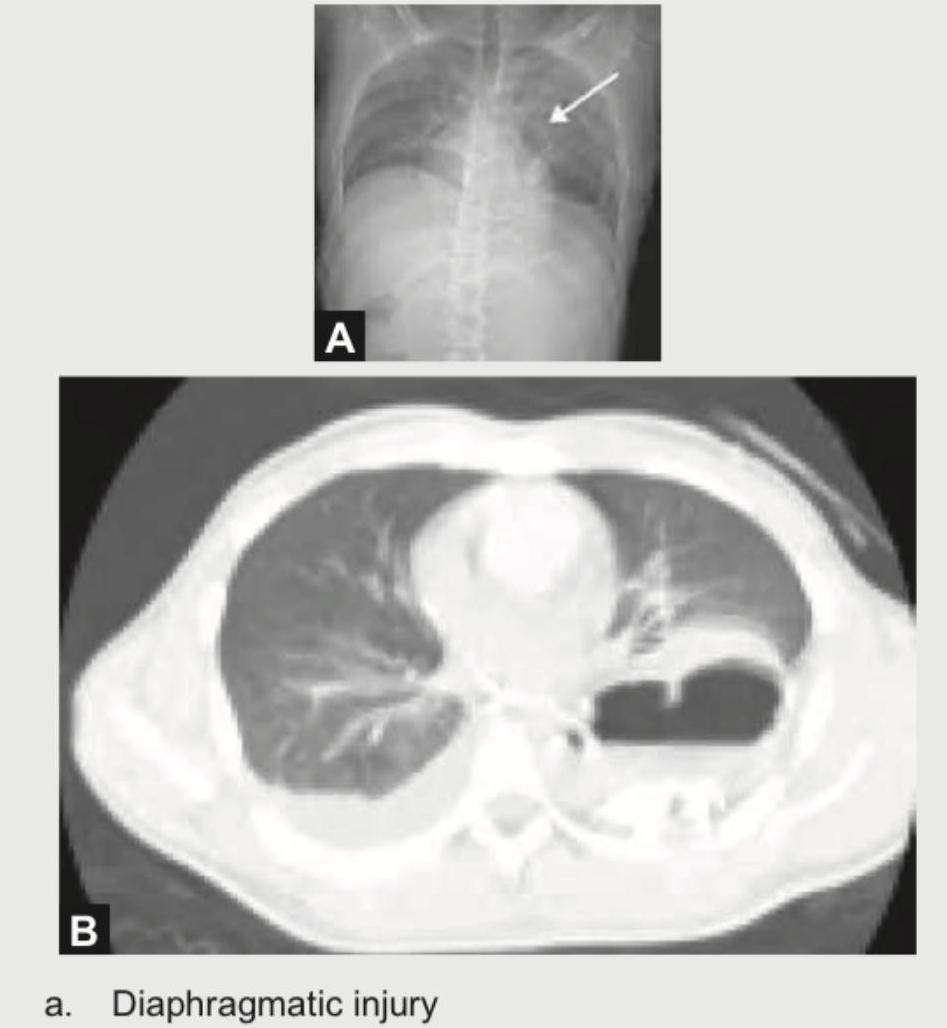
A 25-year-old corporate executive was stabbed in the abdomen in a discotheque. In the emergency room, CXR and CT chest were performed. The radiologist then put an NG tube in the patient, injected contrast and repeated the scan. What is the diagnosis?
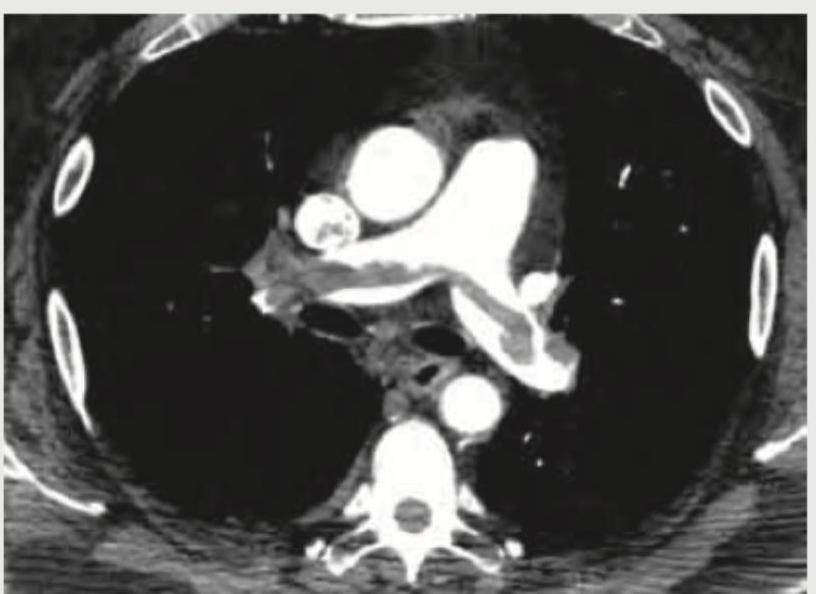
A 35-year-old male with history of 4 weeks of immobilization for fracture of femur develops sudden onset breathlessness and blood in sputum. CT angiography shows? (Recent NEET Pattem 2018-19)
Which one of the following statements is correct regarding eFAST in trauma? 1. It is a technique to assess free fluid in abdominal cavity, thoracic cavity, and pericardium. 2. It is a technique to assess free fluid in pelvic cavity. 3. It is a technique to assess free fluid in pleural cavity. Select the correct answer using the code given below:
In an unconscious patient with multiple injuries, what is the best and reliable modality for assessment of cervical spine injury?
Practice by Chapter
Trauma Imaging Protocols
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Trauma Imaging
Practice Questions
Chest Trauma Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Musculoskeletal Trauma Imaging
Practice Questions
Non-traumatic Neurological Emergencies
Practice Questions
Non-traumatic Thoracic Emergencies
Practice Questions
Non-traumatic Abdominal Emergencies
Practice Questions
Vascular Emergencies
Practice Questions
Pediatric Emergency Imaging
Practice Questions
Imaging of Non-accidental Trauma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app