
Emergency Radiology — MCQs

On this page
Whole-body CT scan protocol for a trauma patient includes all, except
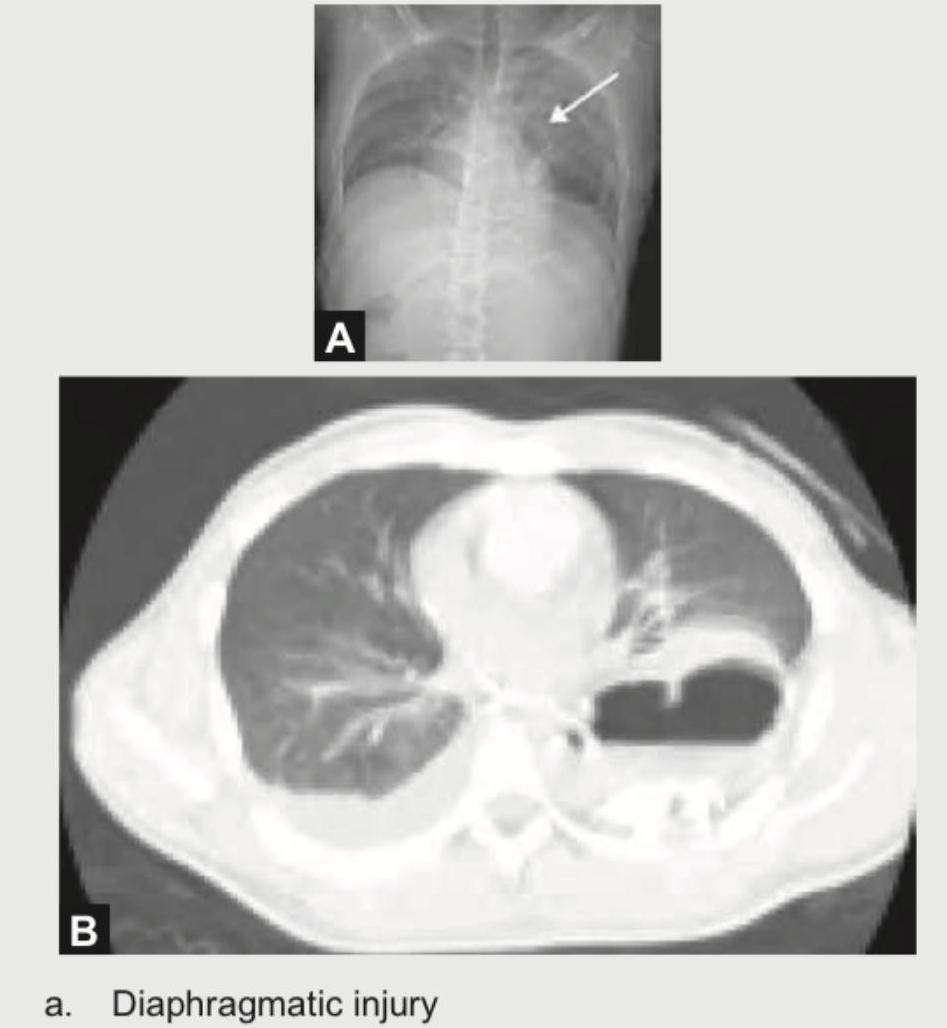
A 25-year-old corporate executive was stabbed in the abdomen in a discotheque. In the emergency room, CXR and CT chest were performed. The radiologist then put an NG tube in the patient, injected contrast and repeated the scan. What is the diagnosis?
In an unconscious patient with multiple injuries, what is the best and reliable modality for assessment of cervical spine injury?
FAST (Focused Assessment with Sonography for Trauma) is used to detect free fluid in which of the following areas?
A 25-year-old patient presents in emergency with abdominal trauma. Why is FAST done?
In a hemodynamically stable patient with abdominal trauma, which imaging modality is considered the gold standard for diagnosing and grading solid organ injuries?
The most appropriate investigation to diagnose and determine the extent of renal injury in a 15-year-old boy who presents with hematuria and left-sided abdominal pain 48 hours after sustaining a blunt abdominal injury, with a pulse rate of 96/minute, blood pressure of 110/70 mmHg, hemoglobin of 10.8 gm%, and packed cell volume of 31%, would be-
Practice by Chapter
Trauma Imaging Protocols
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Trauma Imaging
Practice Questions
Chest Trauma Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Musculoskeletal Trauma Imaging
Practice Questions
Non-traumatic Neurological Emergencies
Practice Questions
Non-traumatic Thoracic Emergencies
Practice Questions
Non-traumatic Abdominal Emergencies
Practice Questions
Vascular Emergencies
Practice Questions
Pediatric Emergency Imaging
Practice Questions
Imaging of Non-accidental Trauma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app