
Non-traumatic Thoracic Emergencies — MCQs

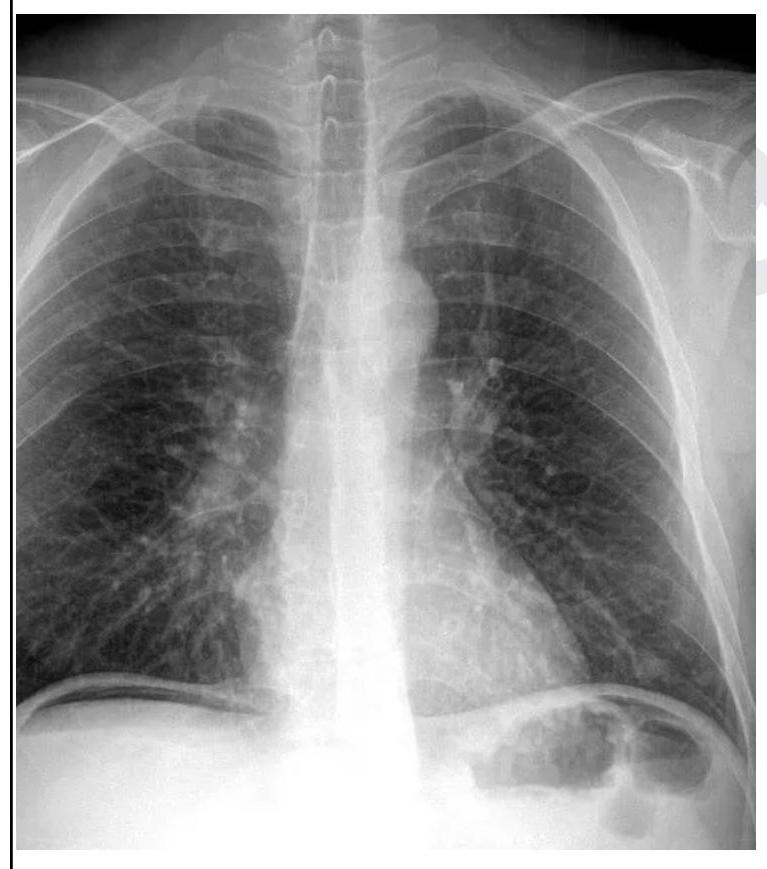
A 26 year old male patient was brought to the emergency department with abdominal pain and obstipation for 3 days. He gives a history of bull gore to the abdomen 3 days back. His chest X-ray is given below. What is the probable diagnosis?
Pulmonary embolism is most commonly produced by which of the following?
IOC for Acute Aortic Dissection in a Clinically Unstable patient is?
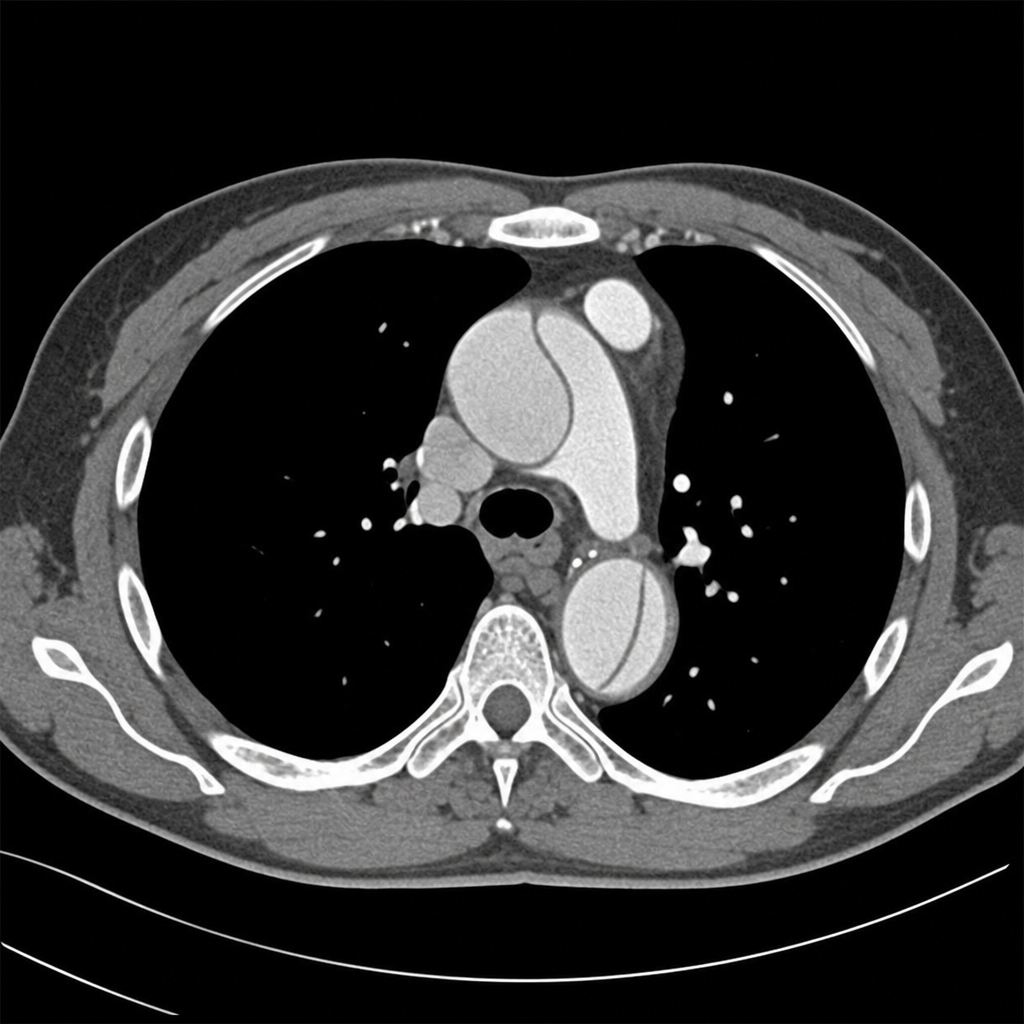
Comment on the diagnosis of the CT chest image shown below.
Which of the following statements about pulmonary embolism is false?
What is a key diagnostic criterion for acute respiratory distress syndrome (ARDS) in a child?
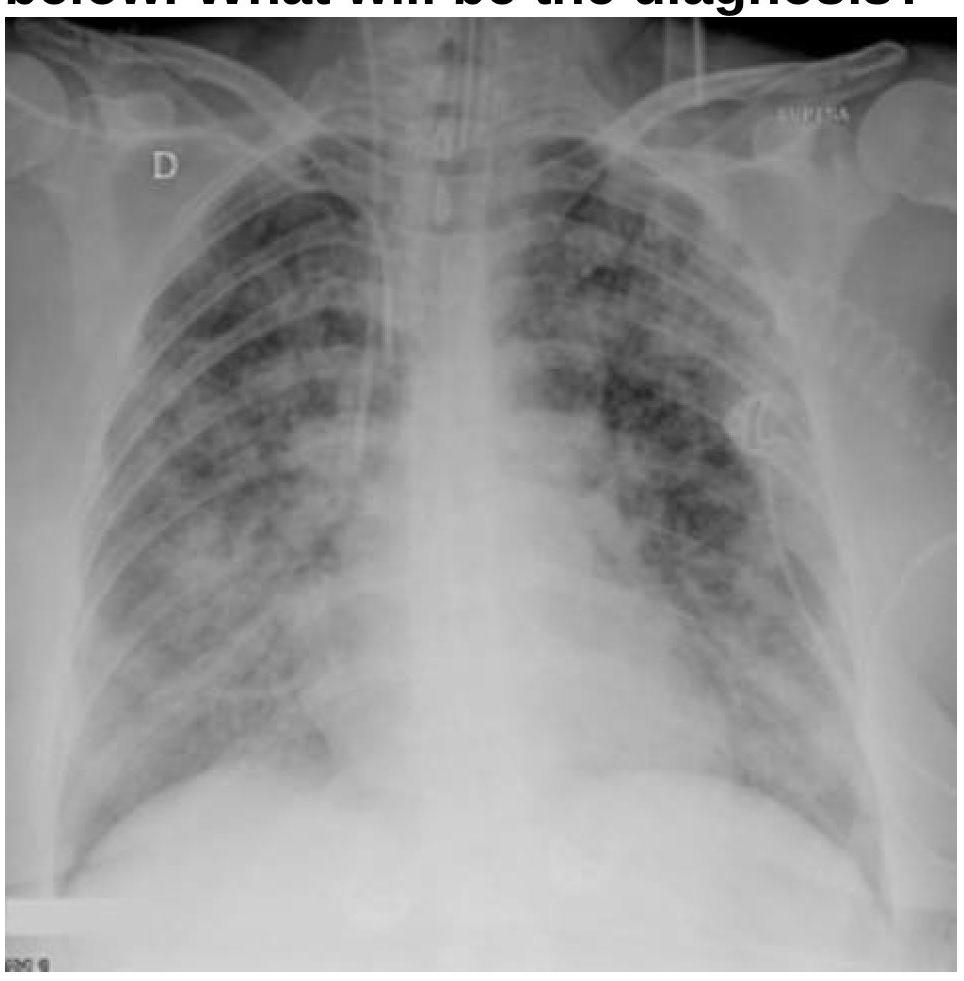
A patient with a known case of acute pancreatitis develops breathlessness and bilateral basal crepitations on day 4. What is the most likely diagnosis based on the chest radiography image?
A Patient presented to emergency with multiple rib fractures. He is conscious speaking single words. On examination, respiratory rate was 40/minute and BP was 90/40 mmHg. What is immediate next step?
Which of the following is shown in the image below?
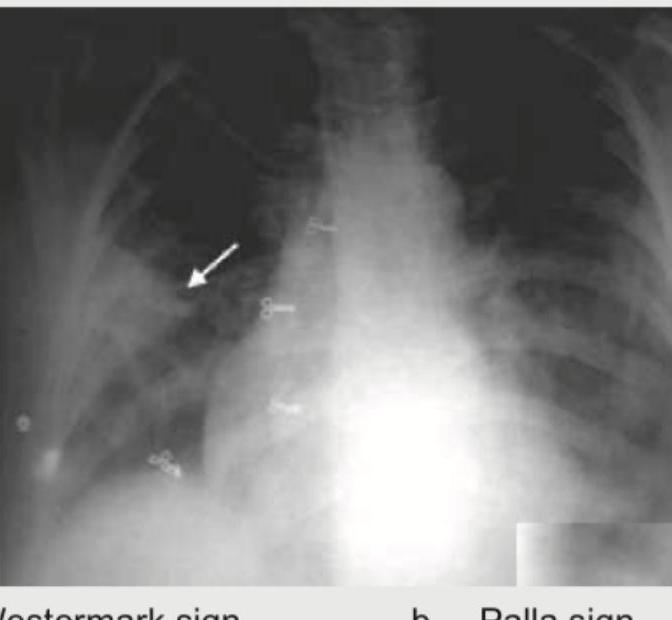
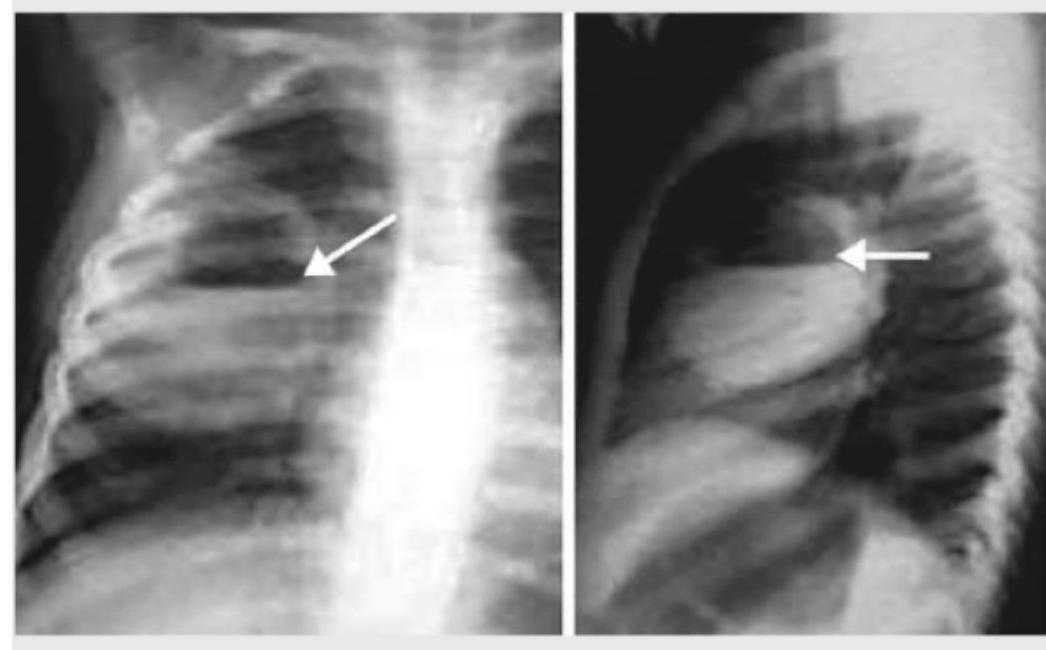
What is the most likely diagnosis based on the chest radiographs shown below?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app