
Non-traumatic Abdominal Emergencies — MCQs

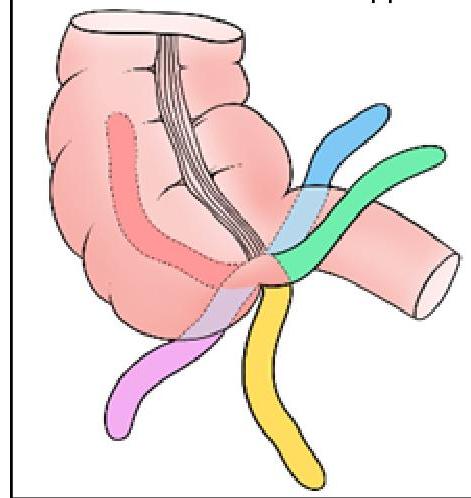
Identify the position of the appendix marked in BLACK in the given image:
Investigation of choice in an unstable patient with suspected intra-abdominal injury is -
Which of the following is the most common cause of acute mesenteric ischemia?
Which of the following is a complication of gallstones?
The coffee bean appearance on imaging is specifically associated with which condition?
Thumb print sign in a plain X-ray is seen in:
A man comes to the emergency department with stab injury to left flank. He has stable vitals. What would be the next step in management?
Most sensitive investigation for abdominal trauma in a hemodynamically stable patient is-
A 29 year old woman presents in emergency ward with amenorrhea of 6 weeks and pain. Urine pregnancy test shows positive. Examination shows diffuse significant lower abdomen tenderness. The pelvic examination is difficult to accomplish due to guarding. Her Beta-hCG level is 4000 mIU/ml. Transvaginal ultrasound shows no pregnancy in the uterus and no adnexal mass but moderate fluid in abdomen. Which of the following is the next best step?
Causes of thickened gallbladder wall on ultrasound examination are all except:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app