
Emergency Radiology — MCQs

On this page
A 24-year-old male presents to the emergency department after a road traffic accident. Based on the given CT scan, what is the most likely diagnosis?
What kind of foreign bodies can be detected by MRI?
Which of the following statements is false regarding the role of chest radiography in a patient presenting with acute abdomen?
The "tear drop sign" is characteristic of which of the following conditions?
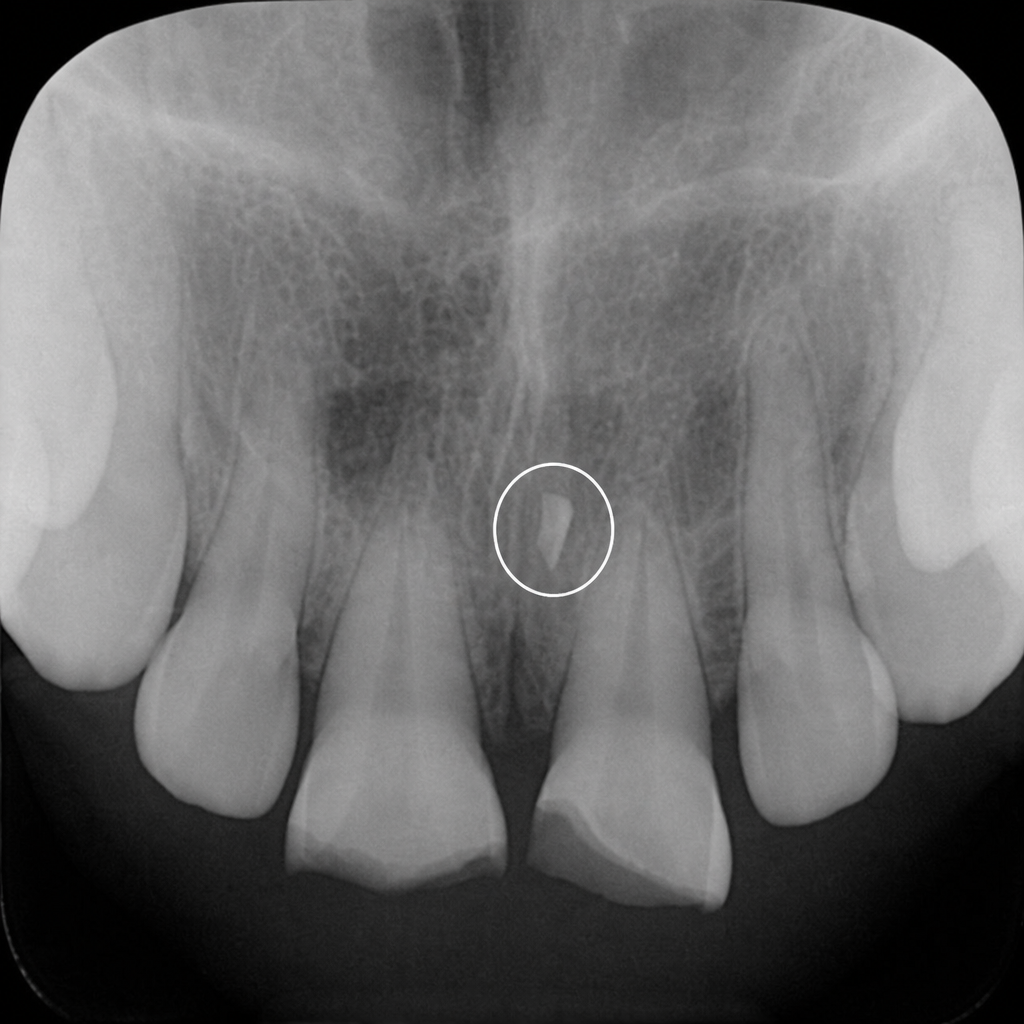
A 19-year-old boy presents with a swollen lip and fractured maxillary central incisors following trauma. The encircled area in the radiograph shows:
Which imaging modality is the mainstay in trauma imaging?
The dependant viscera sign is seen in which of the following conditions?
Which radiographic view best visualizes zygoma fractures?
Pneumocephalus is most commonly seen with fractures of which anatomical structure?
Following a fight between 2 groups, a boy was brought with severe pain in the chest, distended neck veins, dyspnea, and a BP of 80/50 mmHg. X-ray shows the following findings: What is the diagnosis?
Practice by Chapter
Trauma Imaging Protocols
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Trauma Imaging
Practice Questions
Chest Trauma Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Musculoskeletal Trauma Imaging
Practice Questions
Non-traumatic Neurological Emergencies
Practice Questions
Non-traumatic Thoracic Emergencies
Practice Questions
Non-traumatic Abdominal Emergencies
Practice Questions
Vascular Emergencies
Practice Questions
Pediatric Emergency Imaging
Practice Questions
Imaging of Non-accidental Trauma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app