
Contrast and Radiological Procedures — MCQs

On this page
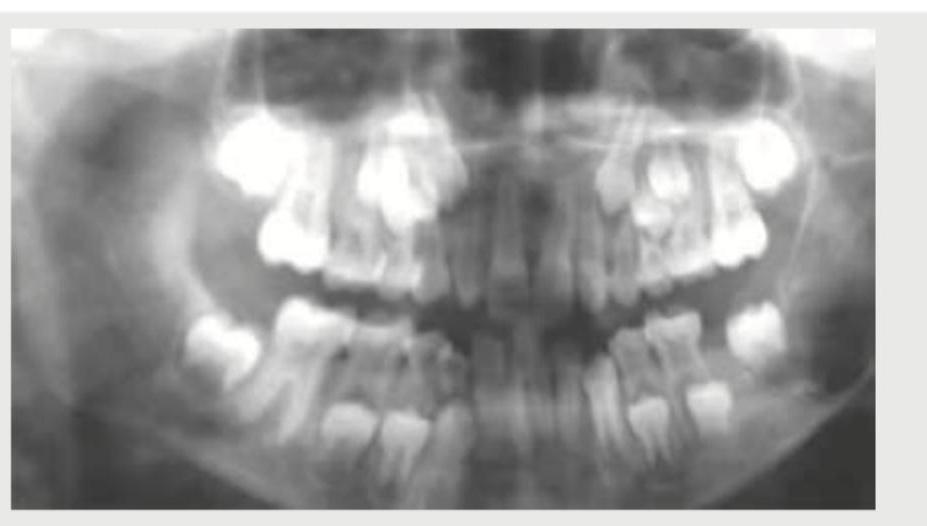
The image shows an intravenous urography (IVU) study with opacification of the renal collecting systems, ureters, and urinary bladder. How is this study performed?
The following image shows:

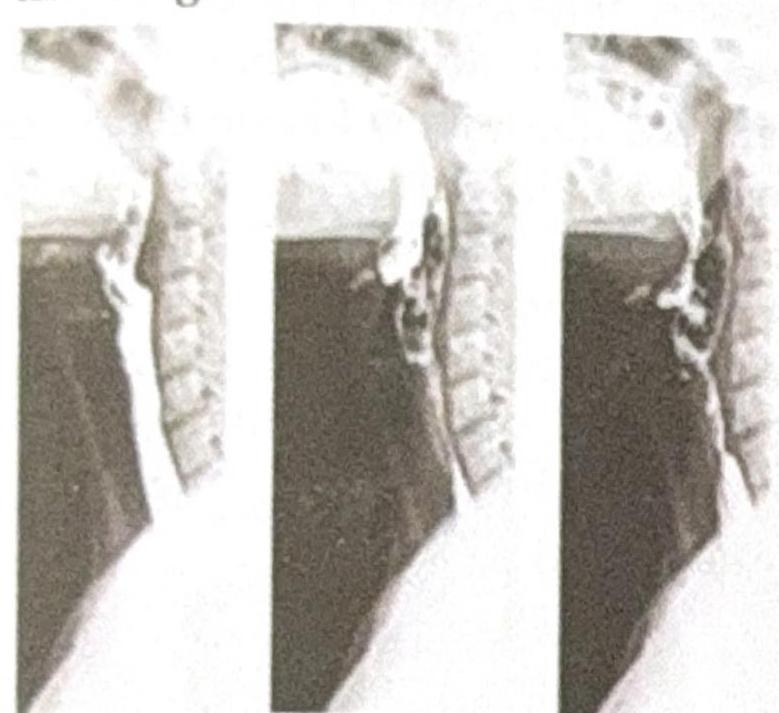
The flow of Barium across the mucosal surface is highly irregular and is seen in which of the following conditions?
The following image shows:
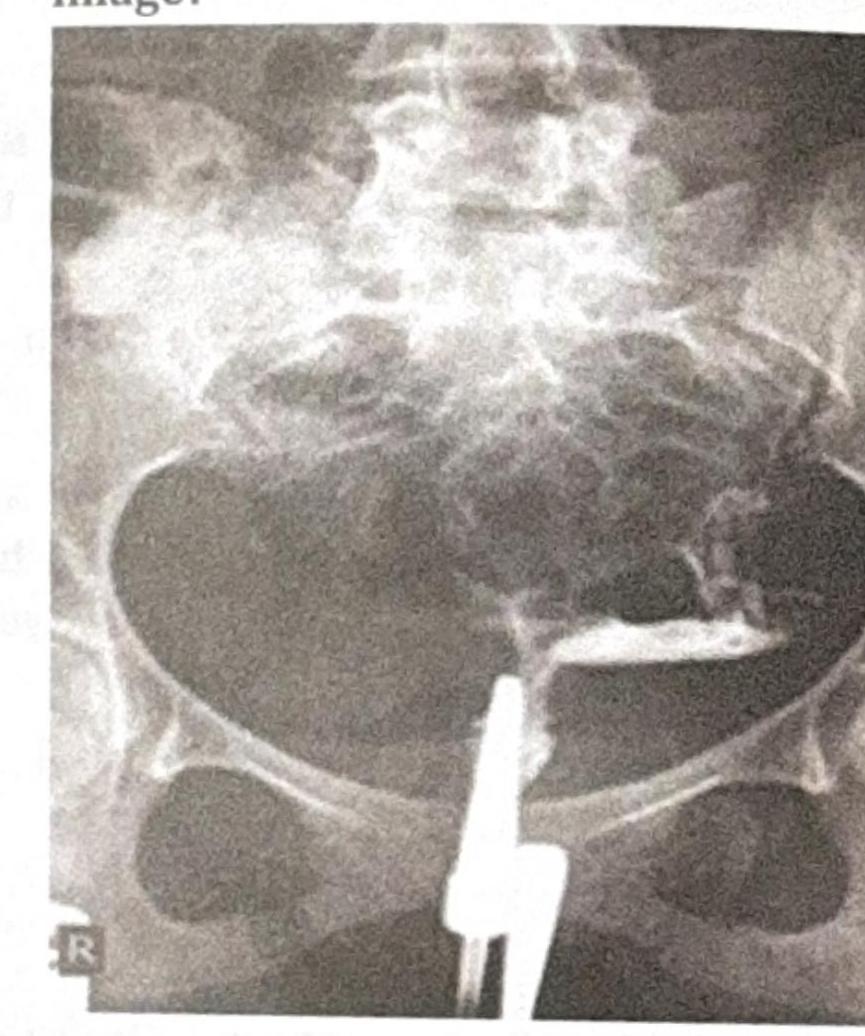
Identify the type of investigation shown in the image below.

Which specific contrast examination is shown in the image?
What is the modality of the test shown in the image?
A 71-year-old man is brought to the emergency department because of severe, progressive left leg pain and tingling for 8 hours. The symptoms began while he was watching television. For several months, the patient has noticed calf cramping when going for long walks, as well as occasional foot tingling and numbness, but did not seek medical attention. He has no history of recent injuries. He has poorly-controlled hypertension, hyperlipidemia, type 2 diabetes mellitus, and osteoarthritis. He smoked one pack of cigarettes daily for 35 years but quit 15 years ago. He drinks three beers every night. Current medications include lisinopril, metoprolol succinate, atorvastatin, metformin, and ibuprofen. He appears to be in severe pain and is clutching his left leg. His temperature is 37.4°C (99.3°F), pulse is 110/min, respirations are 18/min, and blood pressure is 163/94 mm Hg. The lungs are clear to auscultation. There is a harsh II/VI systolic ejection murmur best heard at the right upper sternal border. The abdomen is soft and nontender. The left leg is cool to the touch with decreased popliteal, posterior tibial, and dorsalis pedis pulses. There is 5/5 strength on left hip, knee, and ankle testing. The left hip, knee, and ankle show no gross effusion, erythema, or tenderness to palpation. The remainder of the examination shows no abnormalities. Which of the following is most likely to confirm the diagnosis?
The dye used for OCG is:
Second swallowing in barium meal studies is found in-
Practice by Chapter
Iodinated Contrast Media
Practice Questions
MRI Contrast Agents
Practice Questions
Ultrasound Contrast Agents
Practice Questions
Adverse Reactions to Contrast Media
Practice Questions
Management of Contrast Reactions
Practice Questions
Contrast-Induced Nephropathy
Practice Questions
Barium Studies
Practice Questions
Intravenous Urography
Practice Questions
Angiography Techniques
Practice Questions
Lymphangiography
Practice Questions
Contrast Administration Protocols
Practice Questions
Pretesting and Premedication
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app