
Contrast and Radiological Procedures — MCQs

On this page
Which X-ray view is used to visualize the supraorbital fissure?
In the bisecting technique, how should the film be placed relative to the tooth?
A 50-year-old male patient complains of reduced mouth opening. The patient has a history of a Road Traffic Accident (RTA) one week prior. A submentovertex view x-ray was taken which revealed a zygomatic arch fracture. Which of the following is true regarding the central beam in this x-ray?
Dye for myelography is injected in which space?
MRI is contraindicated in patients with which of the following conditions?
MRI is unsuitable for imaging or examining which of the following?
Identify the imaging study shown in the image.
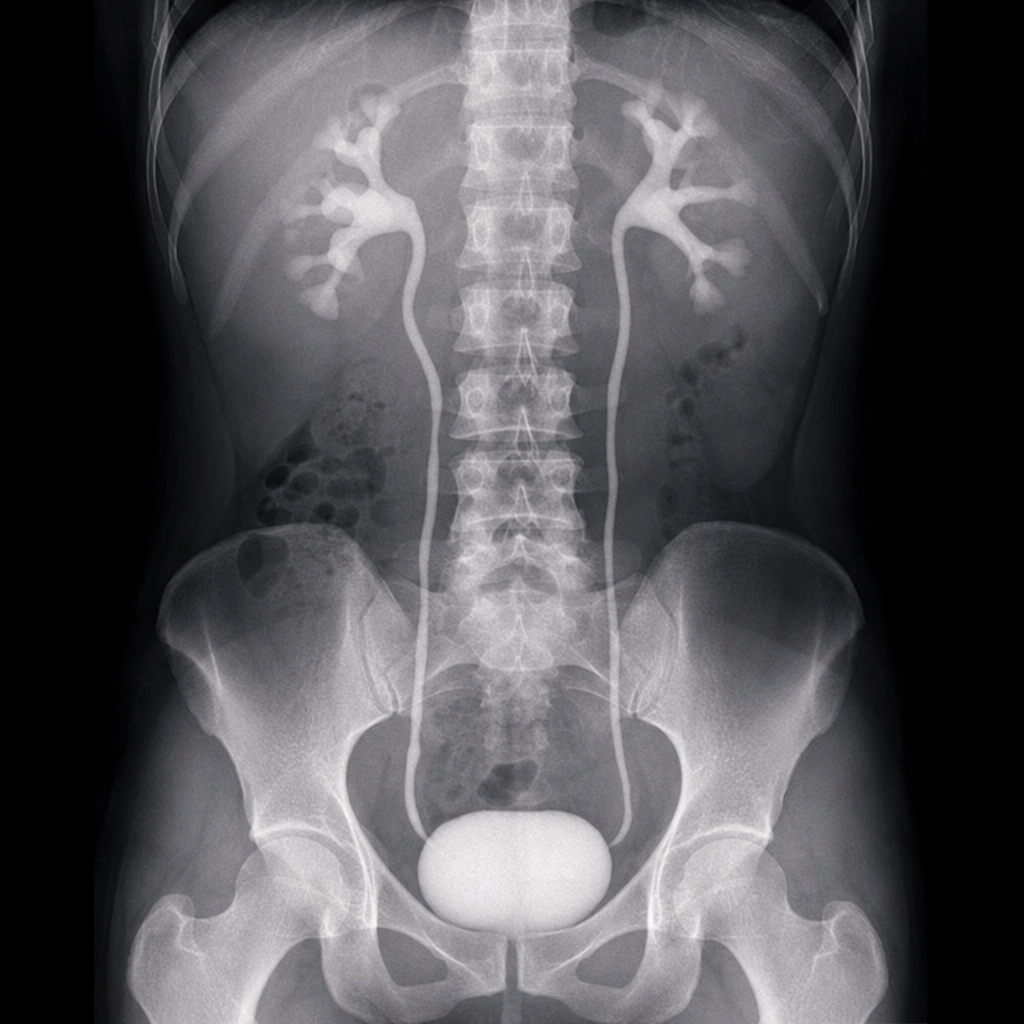
The following radiological image was taken to assess the urinary tract. Identify the investigation shown below.
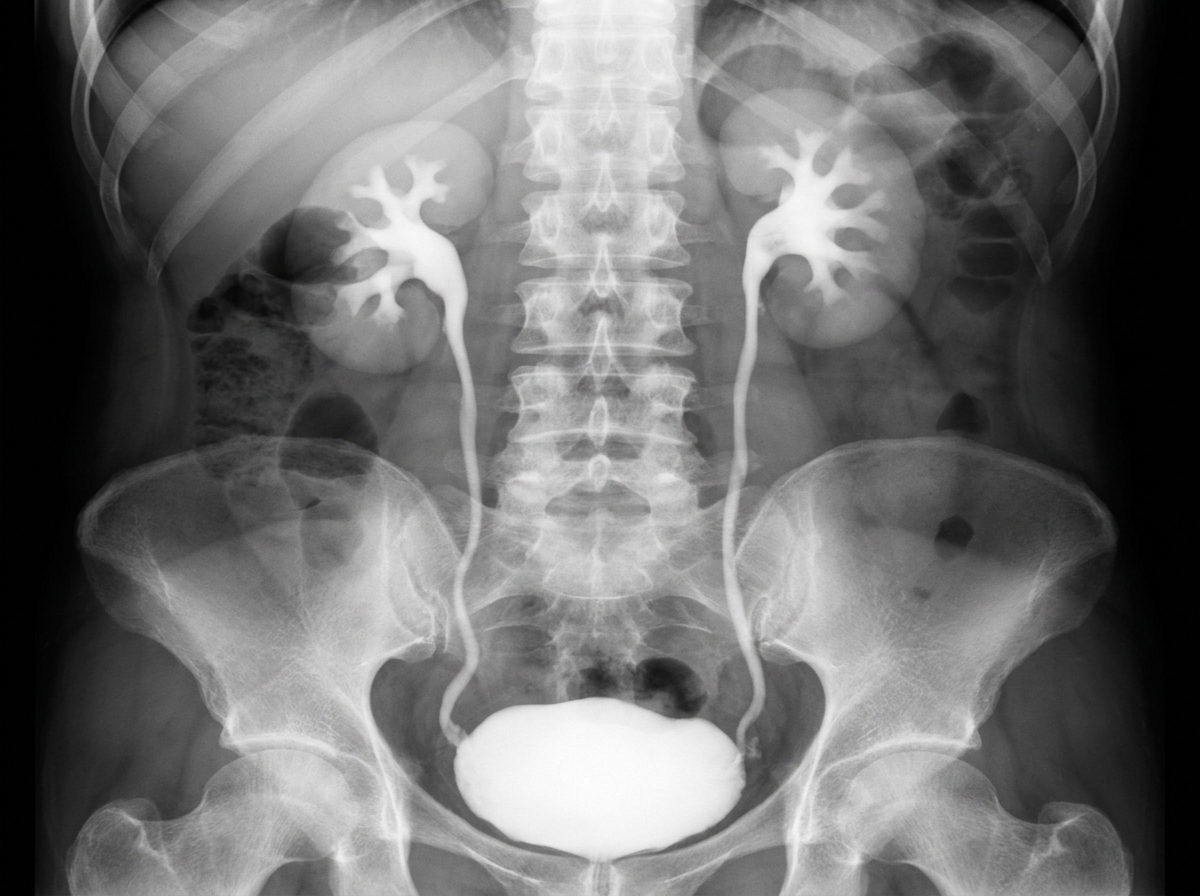
What is the investigation shown in the image?
Identify the procedure shown in the image
Practice by Chapter
Iodinated Contrast Media
Practice Questions
MRI Contrast Agents
Practice Questions
Ultrasound Contrast Agents
Practice Questions
Adverse Reactions to Contrast Media
Practice Questions
Management of Contrast Reactions
Practice Questions
Contrast-Induced Nephropathy
Practice Questions
Barium Studies
Practice Questions
Intravenous Urography
Practice Questions
Angiography Techniques
Practice Questions
Lymphangiography
Practice Questions
Contrast Administration Protocols
Practice Questions
Pretesting and Premedication
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app