
Contrast and Radiological Procedures — MCQs

On this page
Vesicoureteric reflux is diagnosed by which of the following methods?
Which imaging modality is preferred for diagnosing placenta accreta in a 25-year-old pregnant woman at 20 weeks with a history of a previous cesarean delivery?
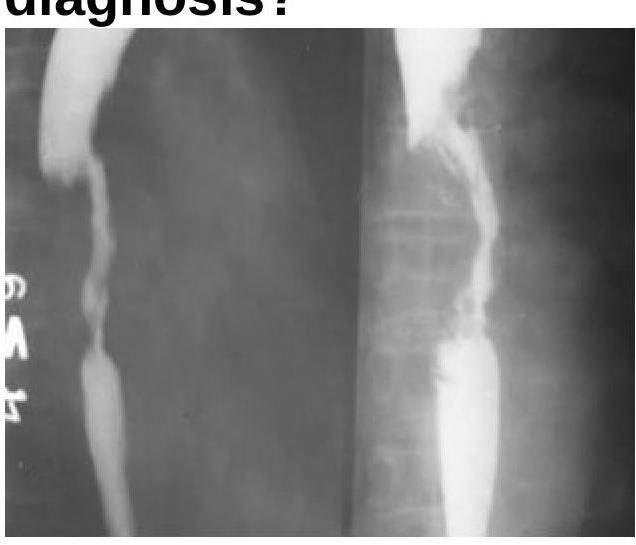
The Barium Swallow examination shows a filling defect in the esophagus. What is the most probable diagnosis?
Barium meal follow through is helpful in diagnosing -
Percentage of renal stones which are radio-opaque:
Early and late suspected instrumental perforation of the oesophagus should first be assessed using?
Which of the following is NOT an indication for a barium meal X-ray?
What is the primary purpose of the Caldwell view in radiology?
A delayed intravenous urogram of a patient is given below. What is the likely diagnosis?

Identify the imaging modality and the location of pathology shown in the image.

Practice by Chapter
Iodinated Contrast Media
Practice Questions
MRI Contrast Agents
Practice Questions
Ultrasound Contrast Agents
Practice Questions
Adverse Reactions to Contrast Media
Practice Questions
Management of Contrast Reactions
Practice Questions
Contrast-Induced Nephropathy
Practice Questions
Barium Studies
Practice Questions
Intravenous Urography
Practice Questions
Angiography Techniques
Practice Questions
Lymphangiography
Practice Questions
Contrast Administration Protocols
Practice Questions
Pretesting and Premedication
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app