
Contrast and Radiological Procedures — MCQs

On this page
What is an X-ray artifact?
Hourglass deformity is seen in which of the following conditions?
Who is credited with inventing the orthopantomographic machine?
The following radiological image was taken to assess the urinary tract. Identify the investigation shown below.
Identify the procedure shown in the image
What is true about the investigation shown below?
The given barium enema is diagnostic of:

The following barium meal shows:
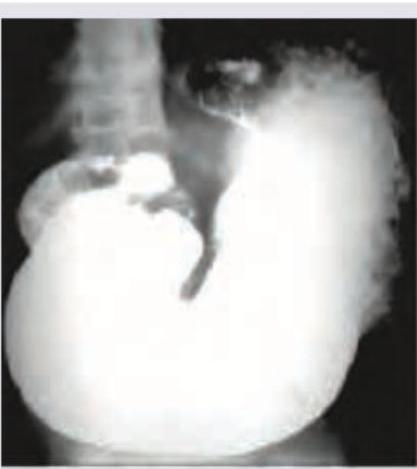
The following image shows:

The flow of Barium across the mucosal surface is highly irregular and is seen in which of the following conditions?
Practice by Chapter
Iodinated Contrast Media
Practice Questions
MRI Contrast Agents
Practice Questions
Ultrasound Contrast Agents
Practice Questions
Adverse Reactions to Contrast Media
Practice Questions
Management of Contrast Reactions
Practice Questions
Contrast-Induced Nephropathy
Practice Questions
Barium Studies
Practice Questions
Intravenous Urography
Practice Questions
Angiography Techniques
Practice Questions
Lymphangiography
Practice Questions
Contrast Administration Protocols
Practice Questions
Pretesting and Premedication
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app