
Chest Radiology — MCQs

On this page
A 35-year-old patient with a history of asbestos exposure presents with chest pain. An X-ray reveals a solitary pulmonary nodule in the right lower zone. A CECT shows an enhancing nodule adjoining the right lower costal pleura with a comet tail sign and adjacent pleural thickening. What is the most likely diagnosis?
Water bottle heart is seen in which of the following conditions?
Westermark's sign, Hampton's hump, and Palla's sign are all characteristic radiological findings suggestive of which condition?
Lucent hemithorax is due to all the following except?
What is not a CT finding in bronchiectasis?
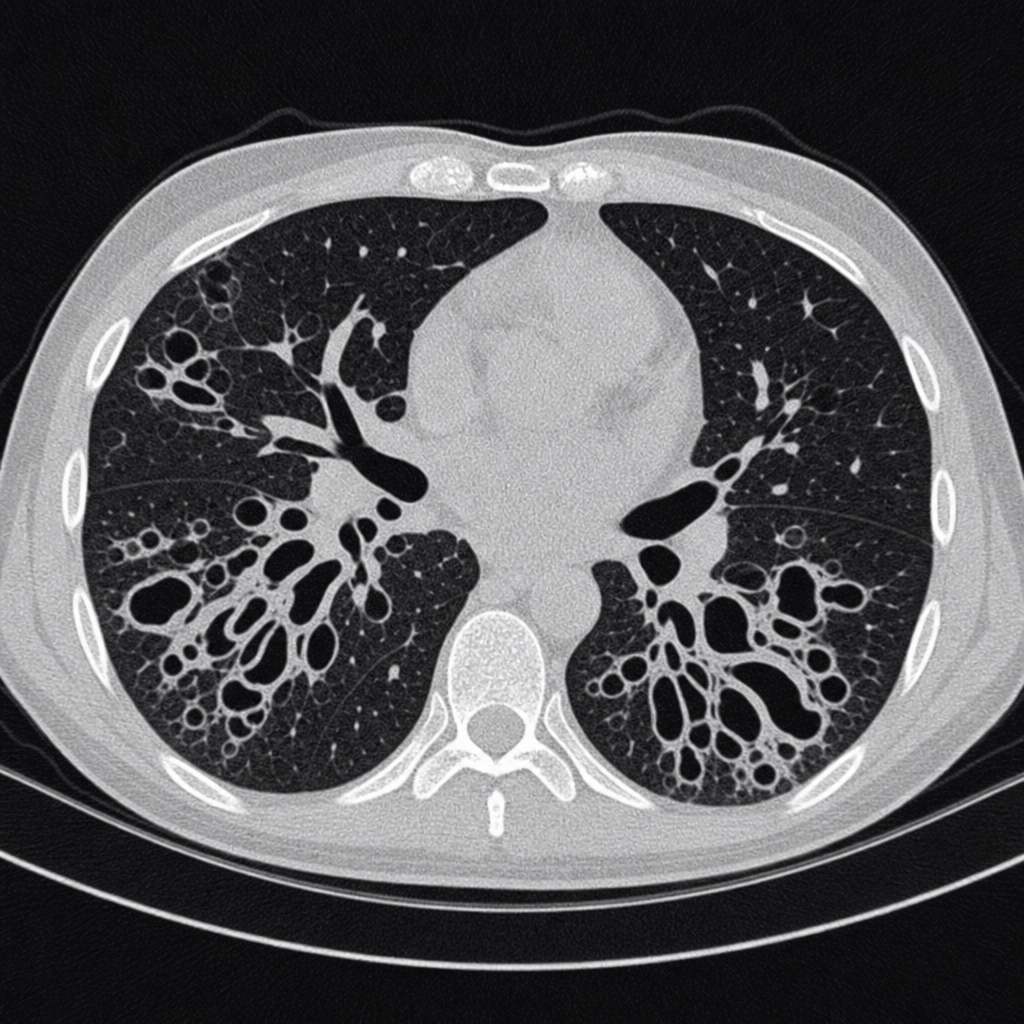
A patient presents with chronic productive cough and clubbing with coarse rales on auscultation. What is the diagnosis suggested by the CT scan findings shown below?
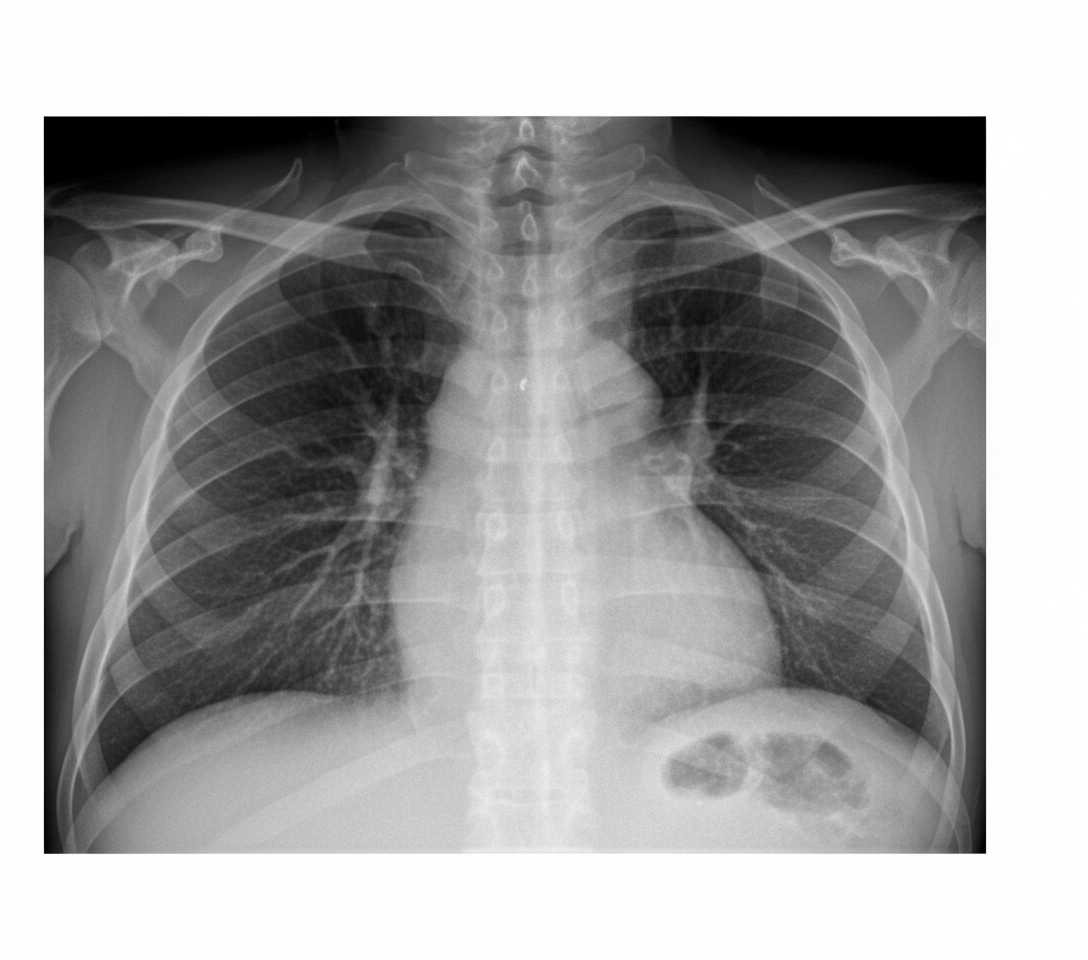
A 42-year-old woman presents with progressive shortness of breath. Cardiac auscultation reveals distant heart sounds, and ECG shows low-voltage QRS complexes. The chest radiograph shown demonstrates mild enlargement of the cardiac silhouette with clear lungs. Which additional finding would most specifically confirm the suspected diagnosis?
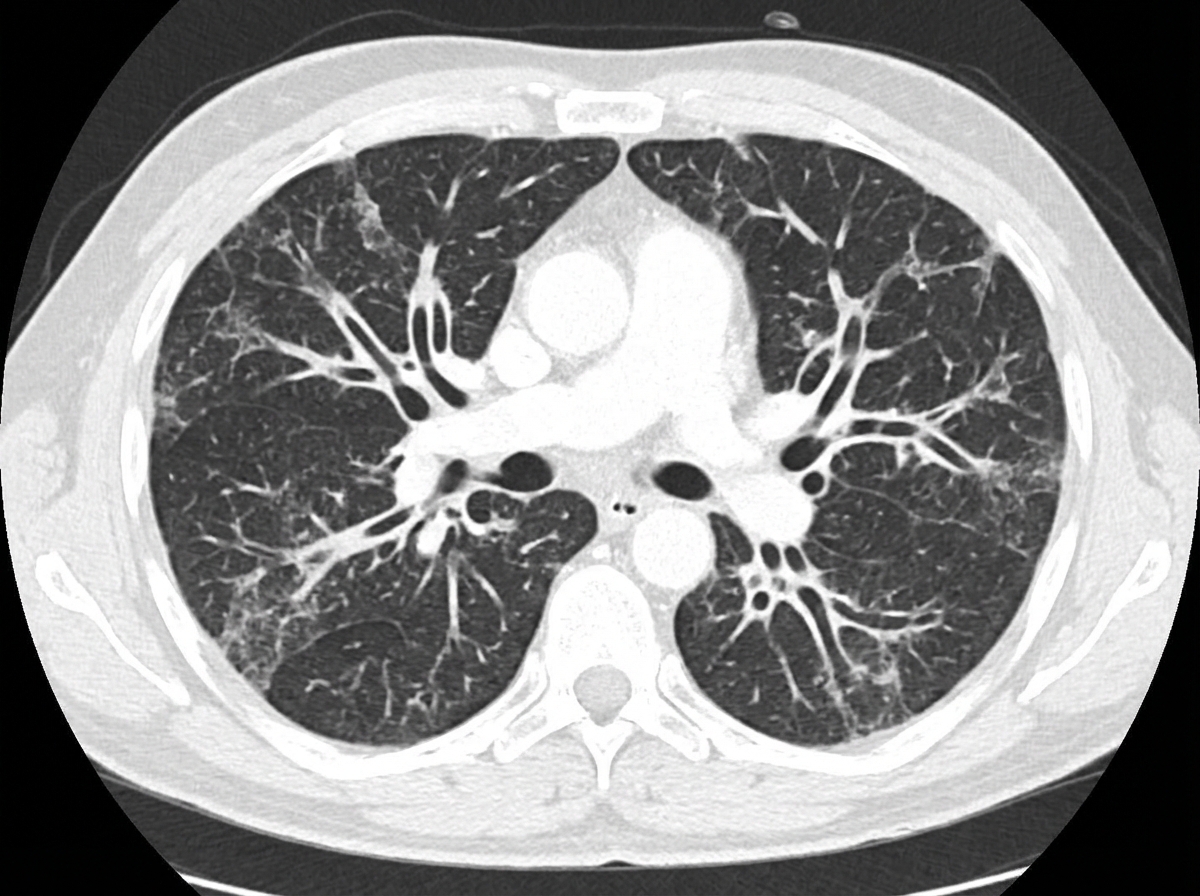
The CT chest of the patient shows the presence of which of the following?
Ground glass appearance is not typically seen in which of the following conditions?
What is the cause of unilateral hypertranslucent hemithorax?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app