
Chest Radiology — MCQs

On this page
A patient presents with a solitary pulmonary nodule on chest x-ray. What is the most appropriate investigation to establish a diagnosis?
Differential diagnosis of a solitary pulmonary nodule includes all of the following except?
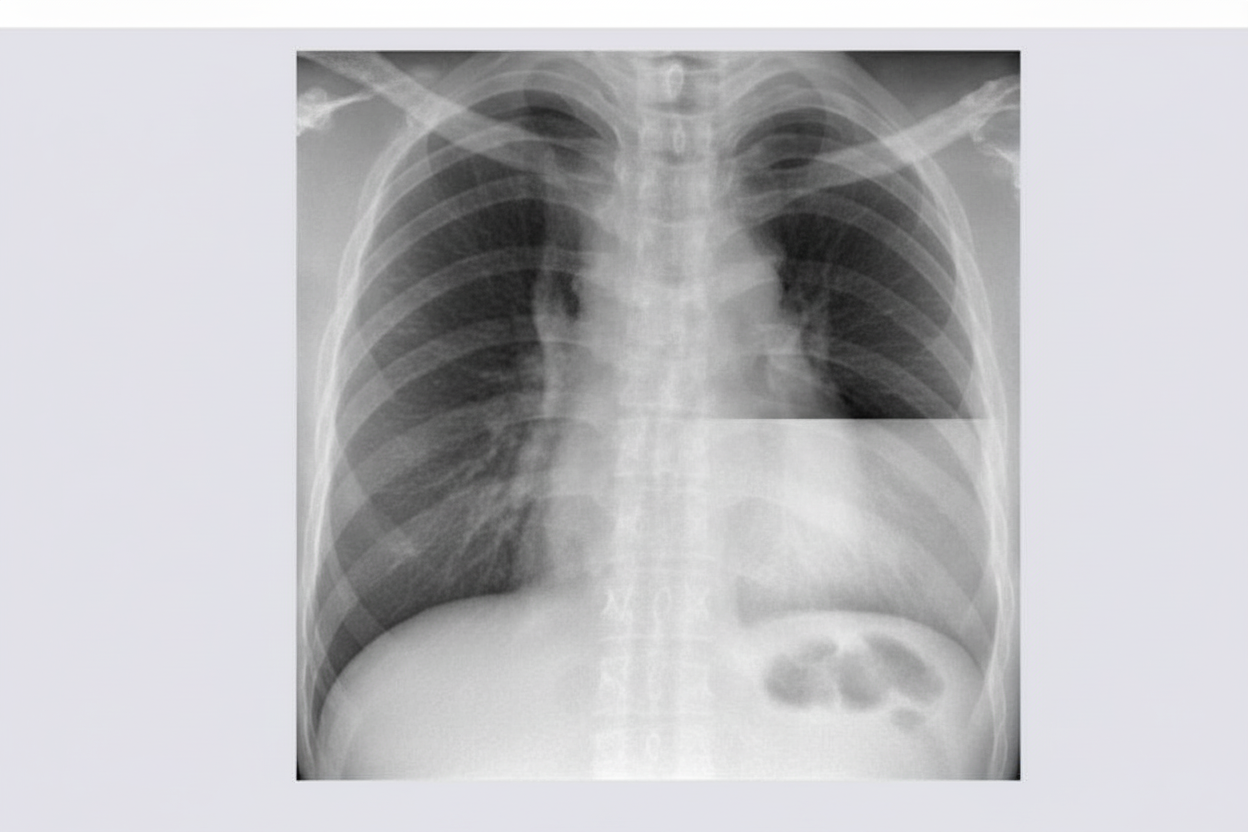
An 81-year-old woman presented with a 1-week history of vomiting. What is the most likely diagnosis?
What does the "sea shore sign" on ultrasound indicate?
What is the most likely diagnosis based on the provided chest X-ray findings?

Pallas sign is seen in which of the following conditions?
The X-ray provided suggests which of the following conditions?
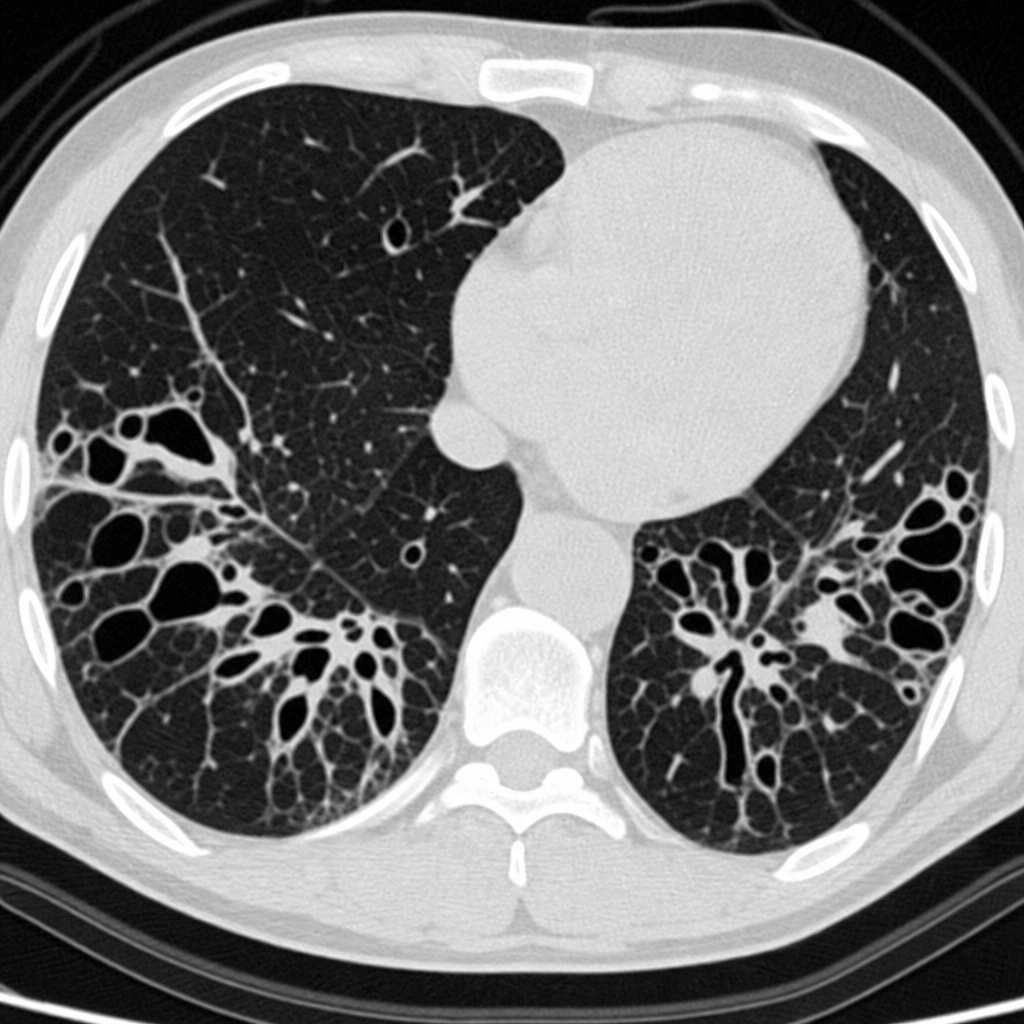
The chest CT scan shown below demonstrates the presence of which of the following findings?
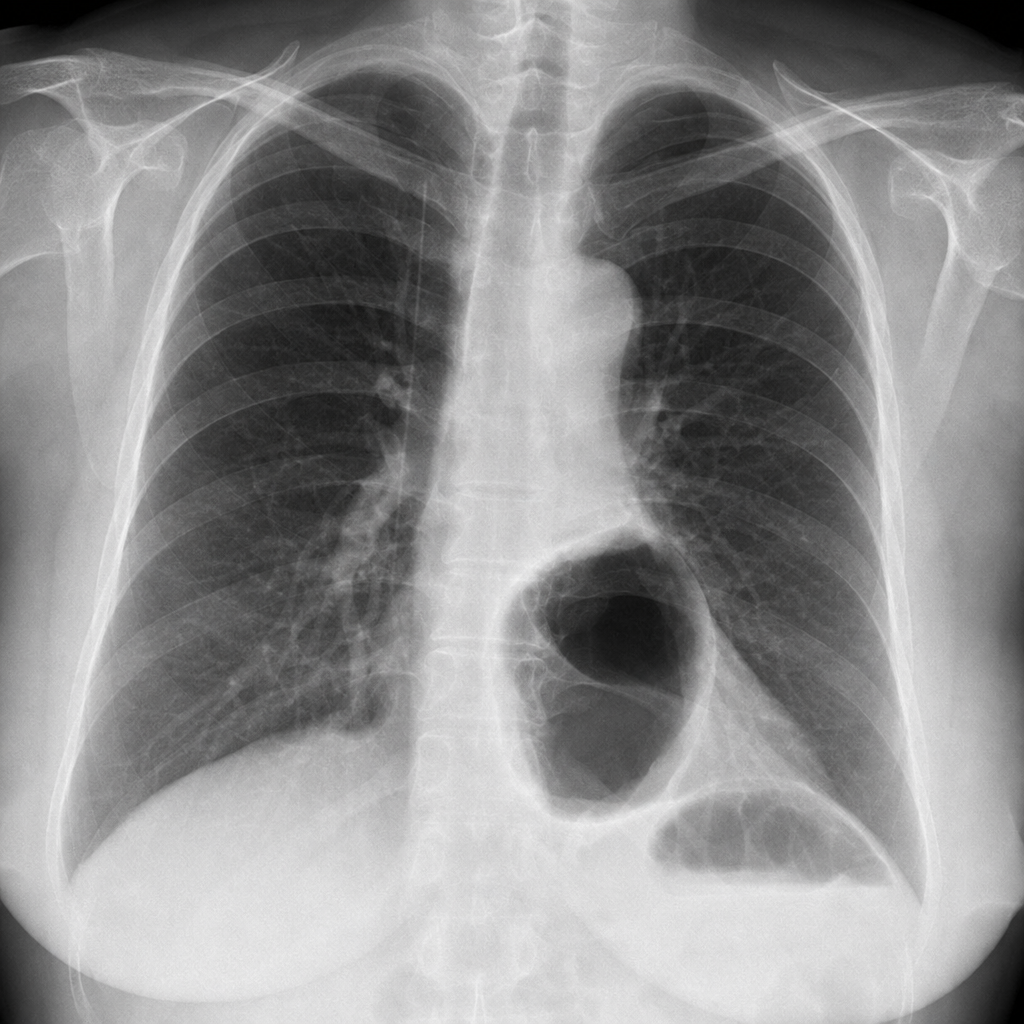
A retrocardiac shadow showing an air-fluid level is seen in which of the following conditions?
The "Golden S" sign is seen in which of the following conditions?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app