
Chest Radiology — MCQs

On this page
The "flat waist sign" is characteristically seen in which of the following conditions?
Which X-ray findings are specific for exposure to asbestos?
A patient presents with cough and fever. On X-ray examination, a homogenous opacity silhouetting the right heart border with ill-defined lateral margins is seen. What is the most probable diagnosis?
Miliary mottling on X-ray chest is seen in which of the following conditions?
Which of the following statements about a normal chest X-ray is true?
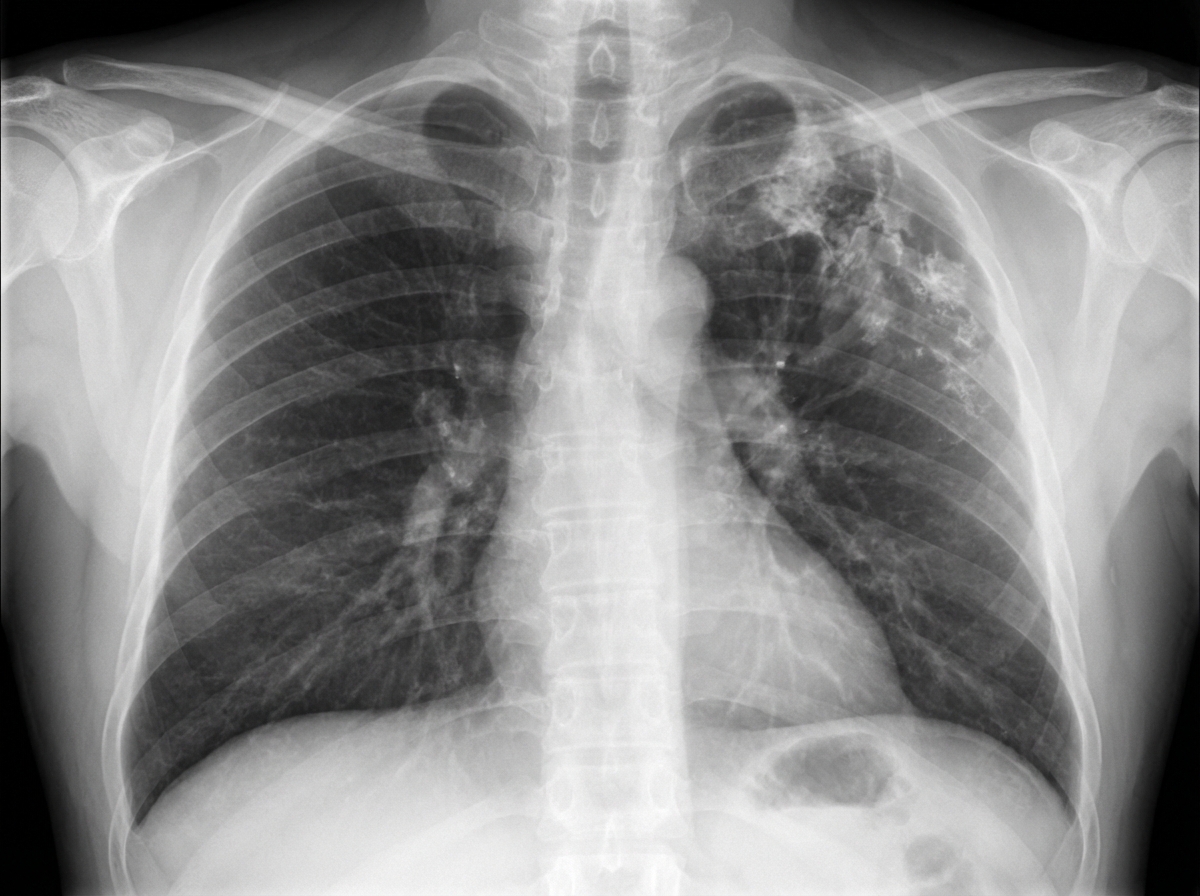
A 68-year-old female smoker presents to the ER with mild hemoptysis and cough, producing 1 to 2 teaspoons of light-green sputum daily. She uses inhalers as needed for occasional shortness of breath. A routine chest X-ray is obtained. What is the most likely cause of the abnormality seen on the CXR?
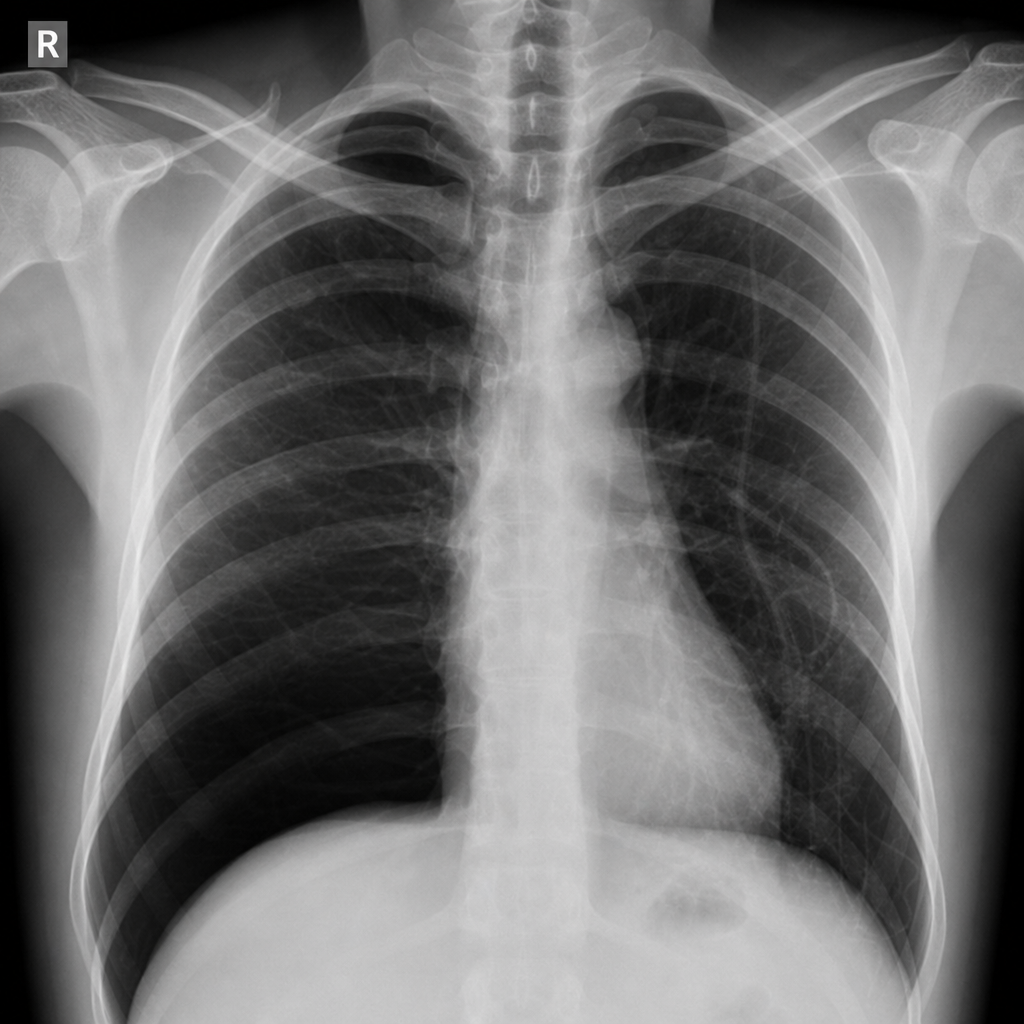
A 30-year-old male chronic smoker presents with progressive breathlessness for 1 month. A chest X-ray is provided. What is the most probable diagnosis?
Which of the following is NOT an X-ray finding of Staphylococcus pneumonia?
Bulging fissures in the lungs is seen in which condition?
All of the following show a miliary shadow on chest X-ray except?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app