
Chest Radiology — MCQs

On this page
Which of the following is NOT a typical finding in left ventricular failure?
What is the initial diagnostic imaging modality of choice for suspected bronchiectasis?
Pulmonary thromboembolism on V-Q scan is suggested by:
Which condition classically presents with an 'apical cap' on a chest X-ray?
The Ellis curve is characteristic of which of the following conditions?
The 'Turkish Sword' appearance is a radiological finding of which of the following conditions?
The "water lilly sign" on a chest X-ray is characteristic of which condition?
All are true about thymus swelling except:
Split Pleura sign is seen in which of the following conditions?
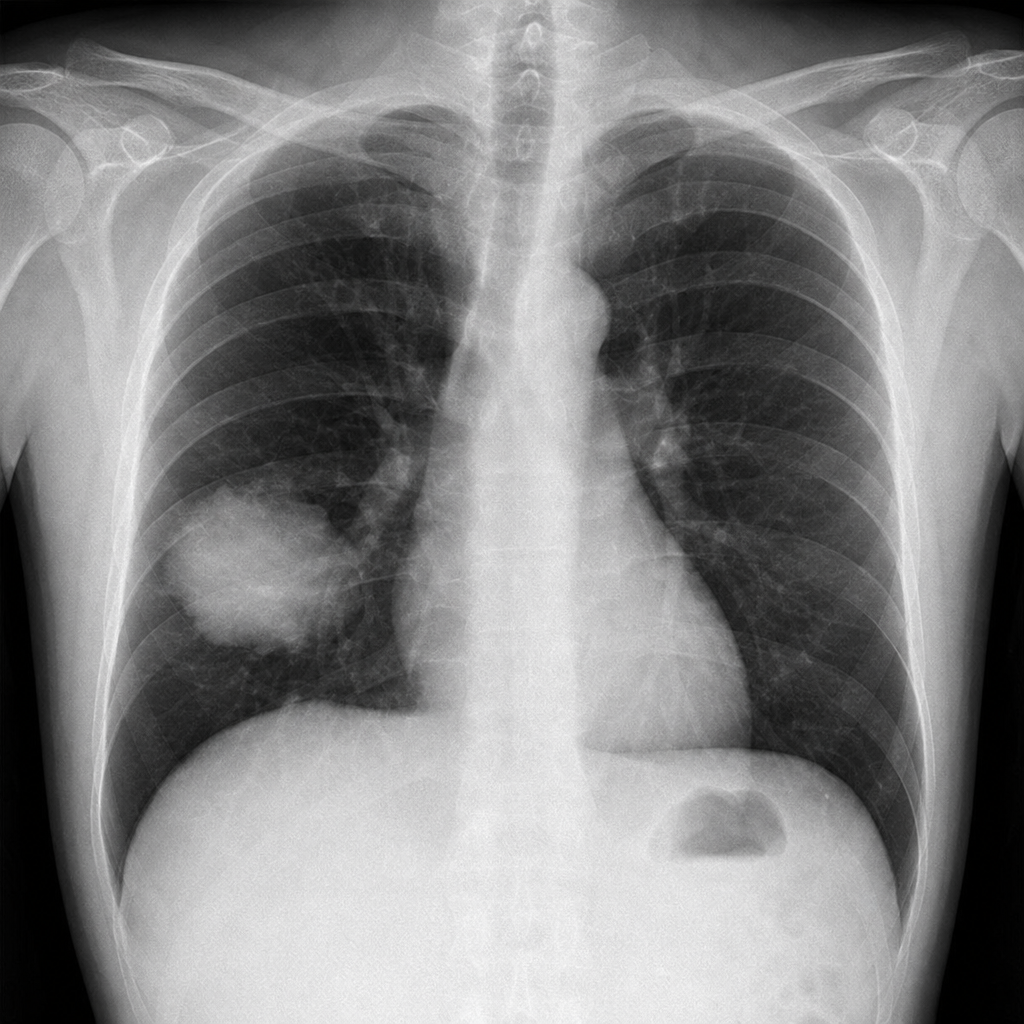
What is the first differential diagnosis for a 50-year-old patient presenting with a cough for two weeks, fever, and chest X-ray showing a round opacity with air bronchograms that resolved after antibiotic therapy?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app