
Chest Radiology — MCQs

On this page
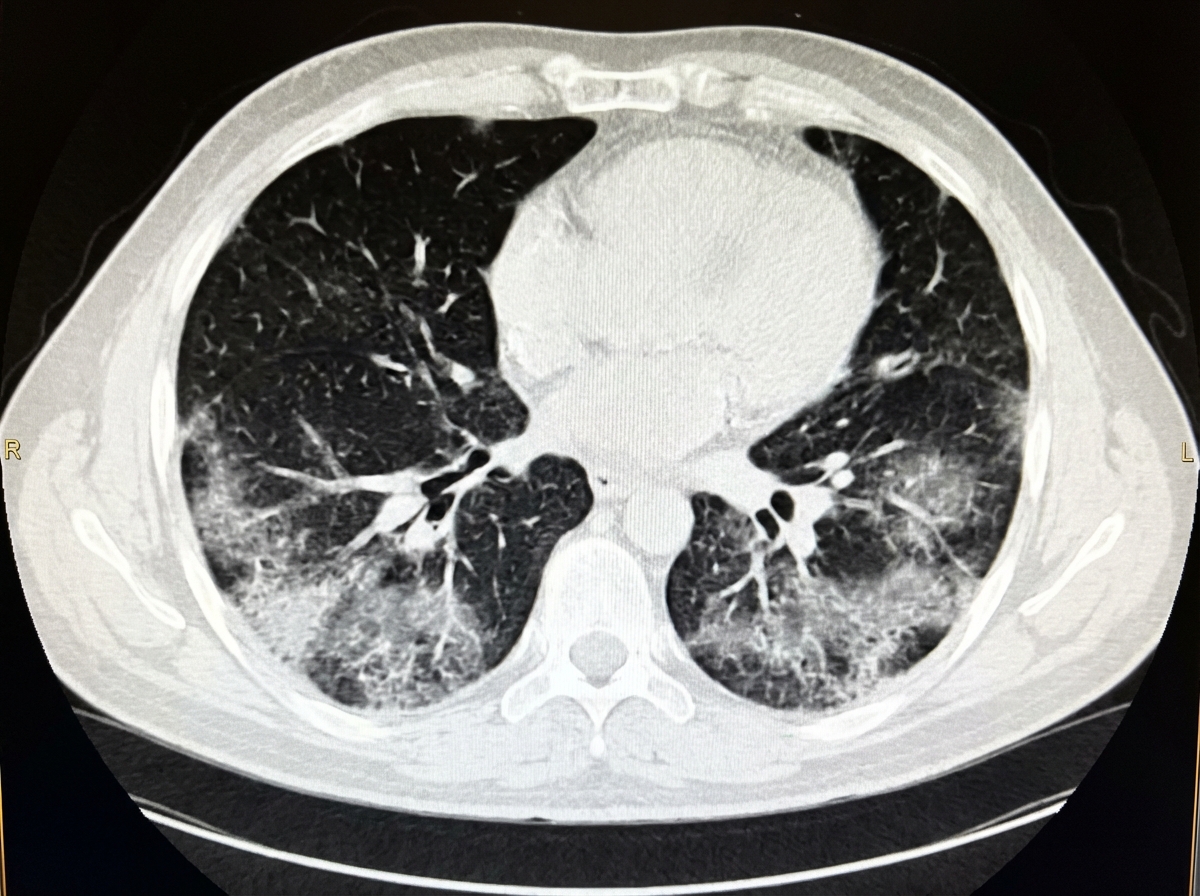
A cruise ship passenger who is a known smoker presents with fever, cough, and shortness of breath for the last 4 days. What do the provided CT chest findings suggest?
Which of the following is NOT a differential diagnosis for a middle mediastinal mass?
Left Pleural effusion is detected best in which position?
A single retrocardiac air-fluid level on a chest radiograph typically implies the presence of what?
Kerley B lines in a chest X-ray are a radiological feature of which of the following conditions?
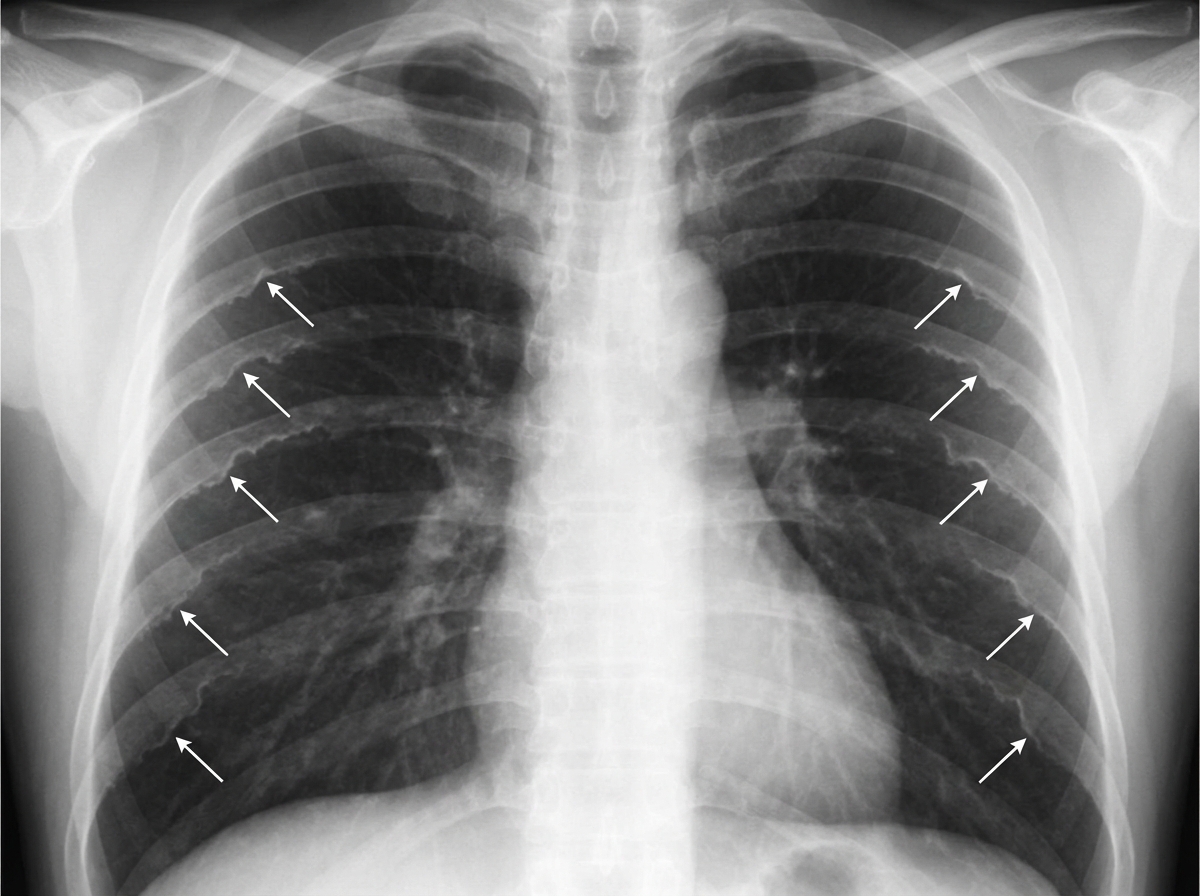
The sign marked by the arrows pointing to the ribs, in the provided chest X-ray, is diagnostic of which of the following conditions?
A 'tear drop heart' is seen in which of the following conditions?
Hilar lymph nodes showing eggshell calcification are seen in all of the following EXCEPT?
What is the best method for detecting minimal bronchiectasis?
The lordotic view is valuable in confirming the presence of a lesion in the lung apex and also in which other location?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app