
Chest Radiology — MCQs

On this page
Inhalational anthrax is characterized by:
Cavitating pulmonary lesions can be seen in the following except:
Which of the following conditions is most commonly associated with eggshell calcifications?
All are radiological features of mitral stenosis except:
Which of the following is the current preferred first-line diagnostic test for pulmonary embolism?
Best diagnostic aid for bronchiectasis is
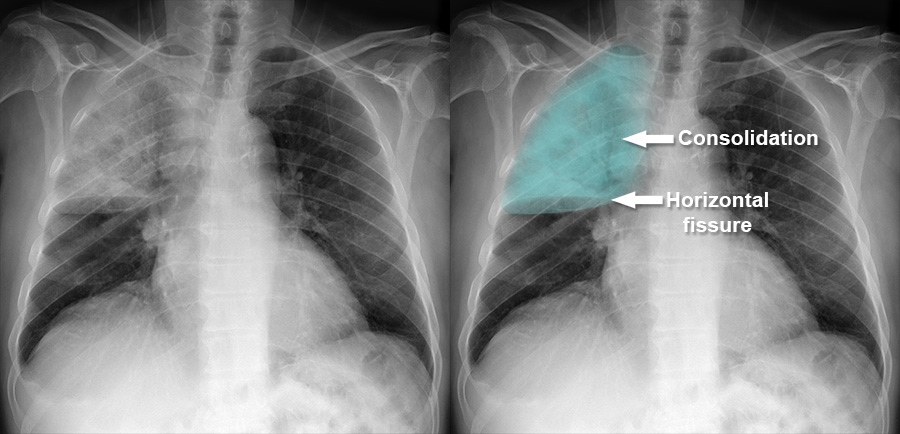
A 70-year-old male presented with complaints of breathlessness and exhibited abnormal bronchial breath sounds on examination. What is the most probable diagnosis based on the provided X-ray image?
Ring sign with dilated bronchi on CXR is a feature of
The following are direct signs of lung collapse seen on a chest X-ray, which one of the following is NOT a direct sign?
Kerley-B lines are seen when pulmonary venous pressure is what?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app