
Chest Radiology — MCQs

On this page
A chest X-ray shows a 'silhouette sign' with opacity obscuring the right heart border. Which lobe of the lung is most likely affected?
Which is NOT a feature of pleural effusion?
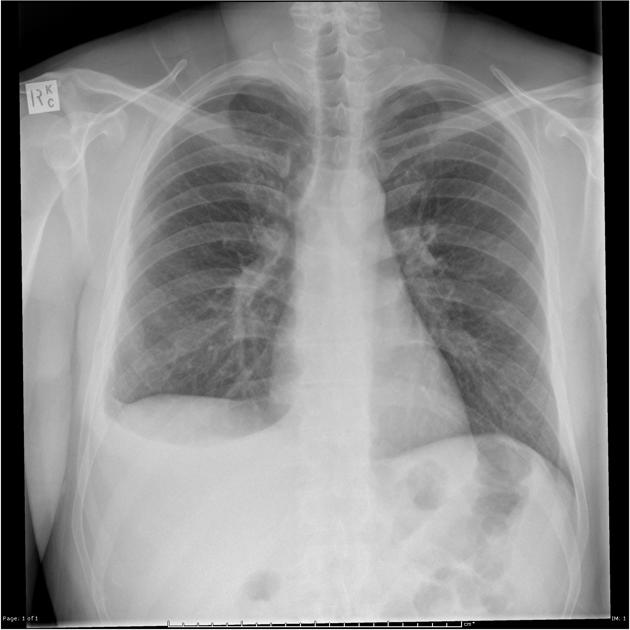
PA view of chest X-ray is given here. What is the diagnosis?

A patient presented with complaints of dyspnoea. The shown X-ray is suggestive of:
Mark the false statement regarding testing of COVID-19.
In a child with coarctation of aorta, all the following are seen in plain chest radiograph except:
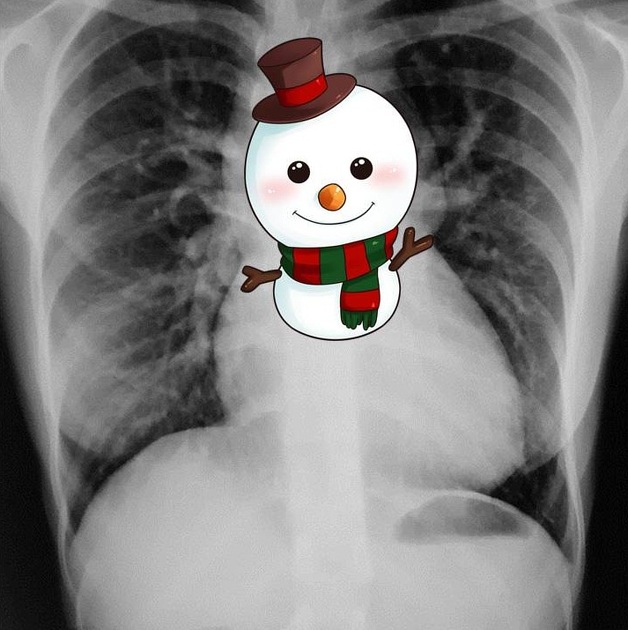
Snowman appearance on x-ray is seen in which cardiac pathology -
A female patient with clinical symptoms of systemic sclerosis presents with shortness of breath and bilateral basal rales. Her chest X-ray showed reticular opacities in bilateral basal fields. What is the next best step?
A patient of Scleroderma presents with acute respiratory distress. Chest X-ray shows B/L reticular basilar shadows. What is the next line of investigation in this patient?
Chest CT shows bilateral ground-glass opacities with crazy paving pattern and preserved bronchial markings. Likely diagnosis?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app