
Chest Radiology — MCQs

On this page
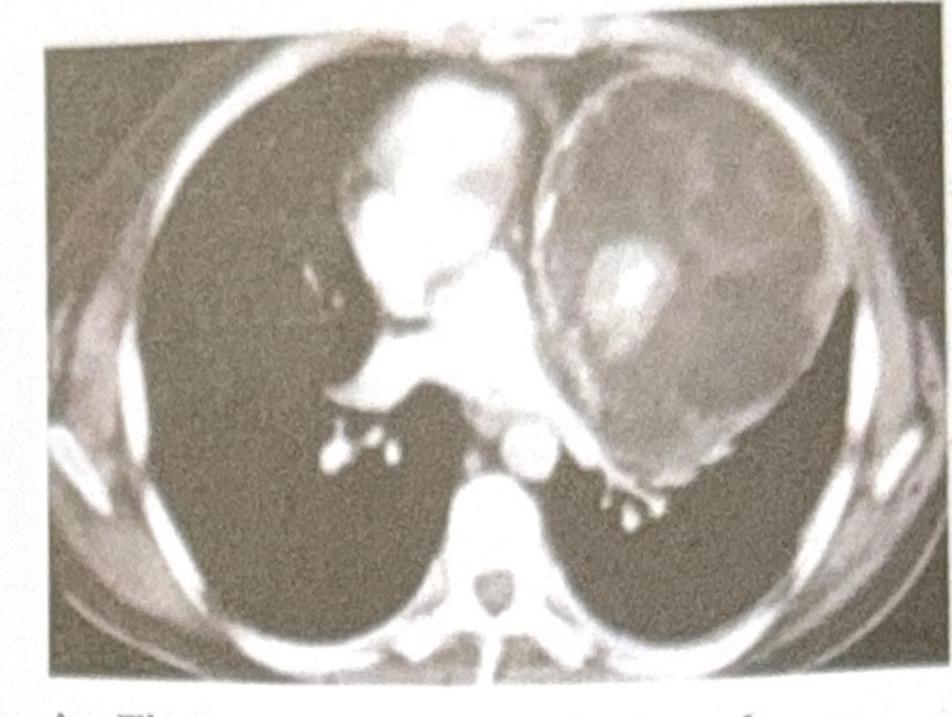
A 25-year-old male presents with chest pain and shortness of breath. A CT scan of the chest is performed, and the image provided shows a large, well-defined mass in the anterior mediastinum. The mass contains both cystic and solid components, along with areas of calcification. Based on the clinical presentation and imaging findings, what is the most likely diagnosis?
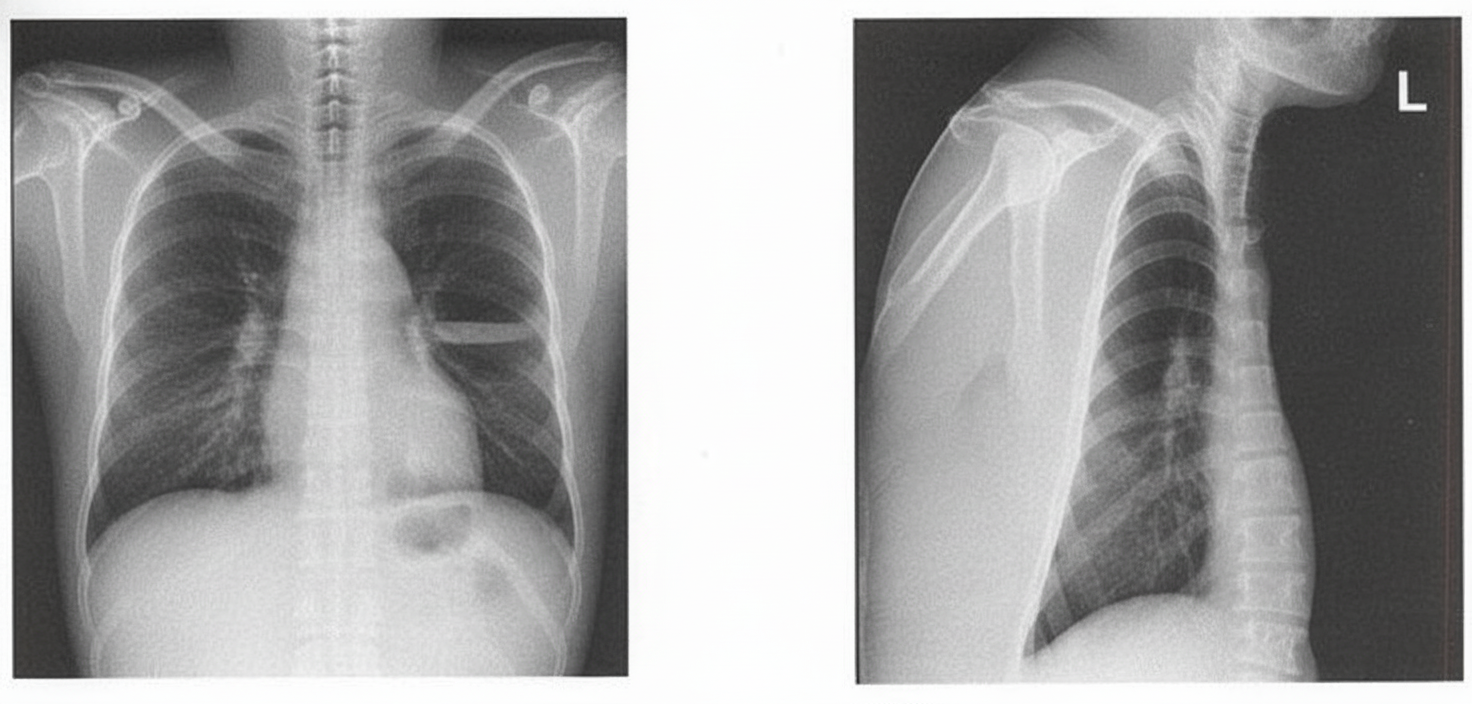
A patient presents with foul-smelling sputum along with breathlessness and fever. Using the X-ray below, identify the diagnosis.
Which of the following findings are seen in a high-resolution CT scan of fungal pneumonia? 1. Interlobular septations 2. Peripheral wedge-shaped consolidation 3. Pleural effusion 4. Cavitatory lesions with surrounding ground glass opacities
A chest CT shows 'doughnut sign' in mediastinum. Which additional finding would best support pulmonary artery sling?
A CT chest shows 'galaxy sign' in lung parenchyma. Which additional finding would best support sarcoidosis?
A chest CT shows 'comet tail' sign in lung bases. Which additional finding would best support rounded atelectasis?
A chest CT shows 'finger-in-glove' sign. Which additional finding would best support allergic bronchopulmonary aspergillosis?
A chest CT shows 'signet ring' sign. Which additional finding would best support bronchiectasis?
A CT pulmonary angiogram shows intravascular webs and bands. Which additional finding would best support chronic pulmonary embolism?
A lung biopsy shows 'temporal heterogeneity' with fibroblastic foci. Which radiological pattern would best support usual interstitial pneumonia?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app