
Chest Radiology — MCQs

On this page
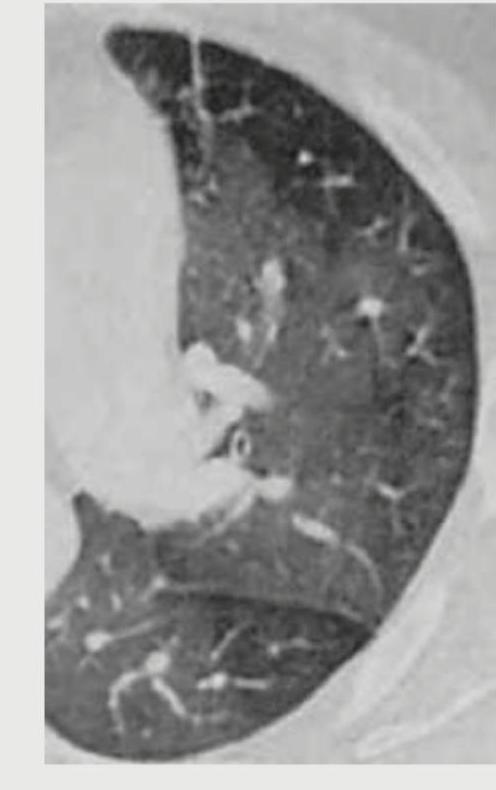
What does the following CT chest show?
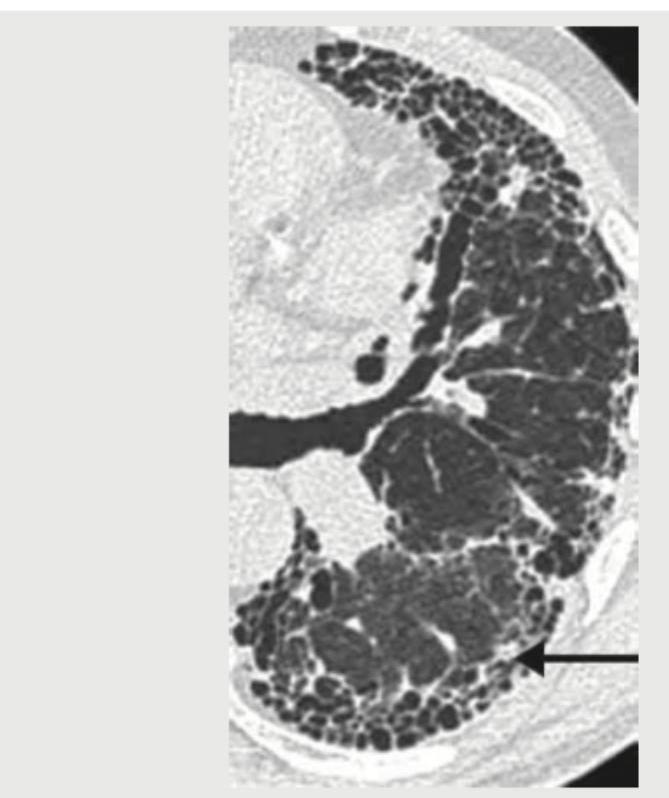
The following lung window in CT chest is taken in which phase of respiration?

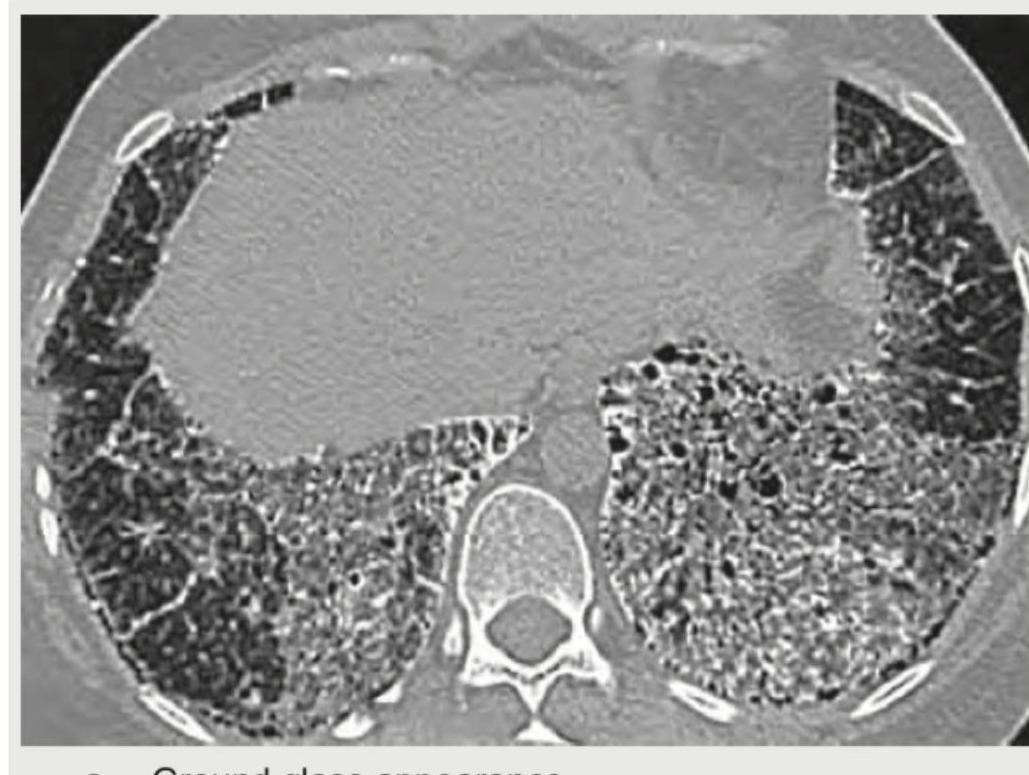
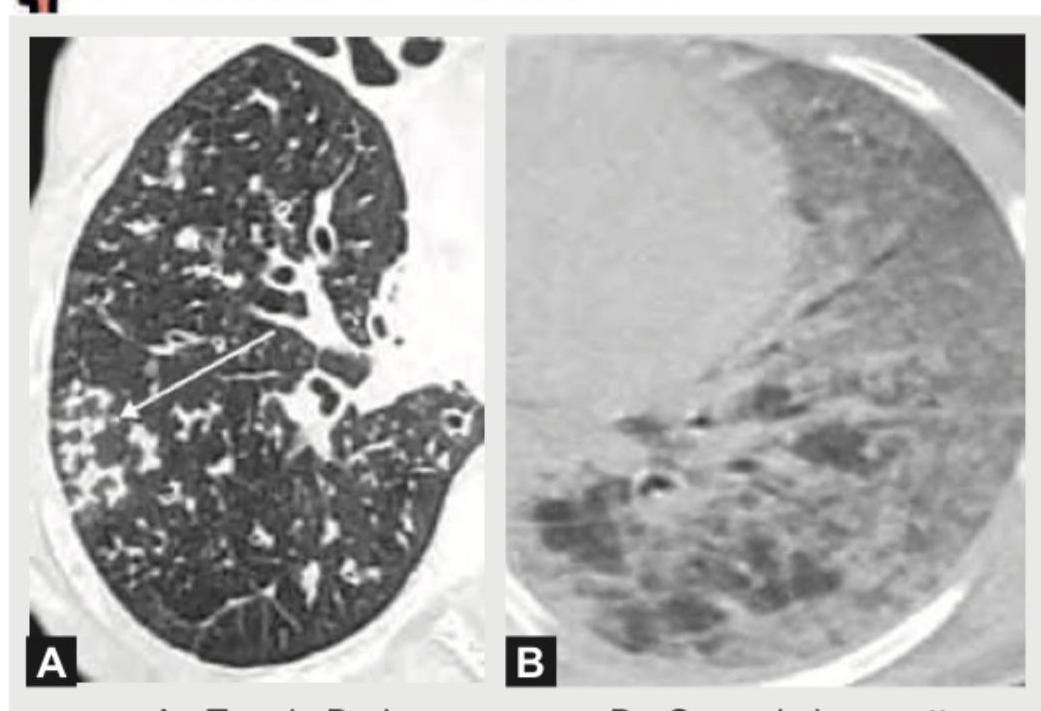
The lung parenchyma on CT chest shown below is best described as:
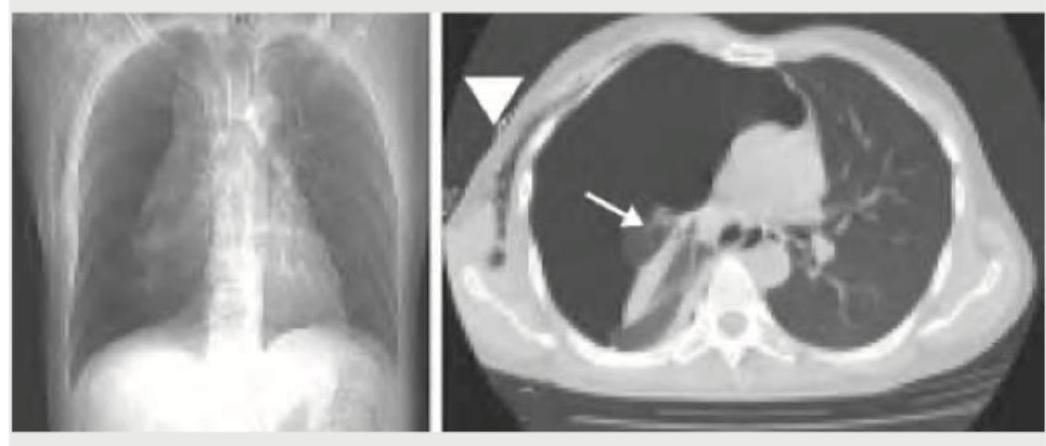
An 18-year-old boy is brought to the hospital with difficulty in breathing after a bar fight. What does the given CT chest show?
What does the following CT chest show?
The following CT chest shows:
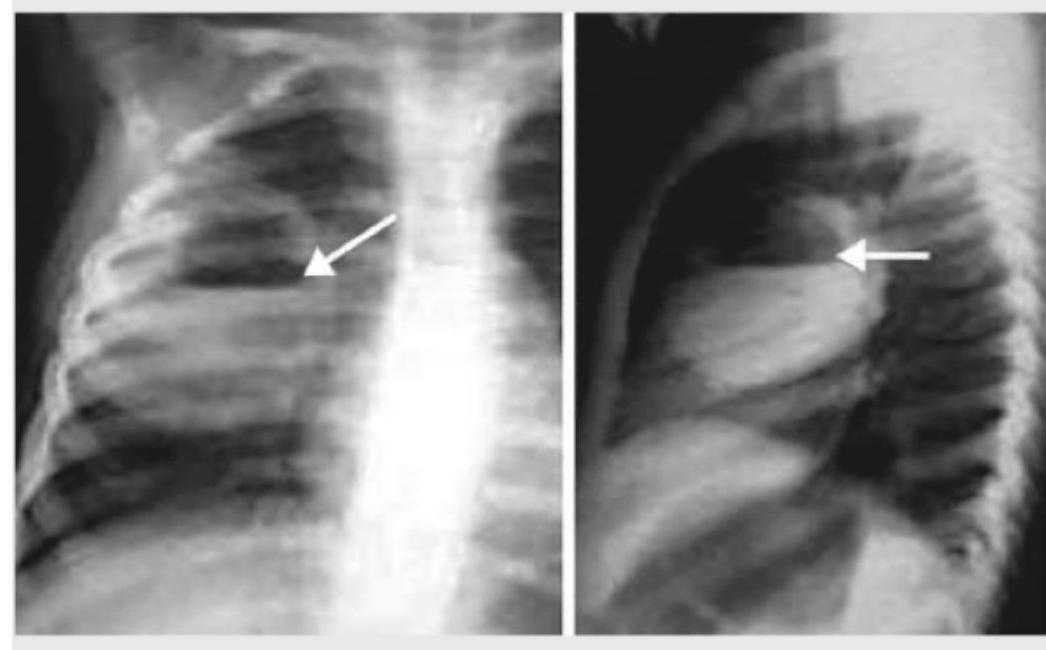
What is the most likely diagnosis based on the chest radiographs shown below?
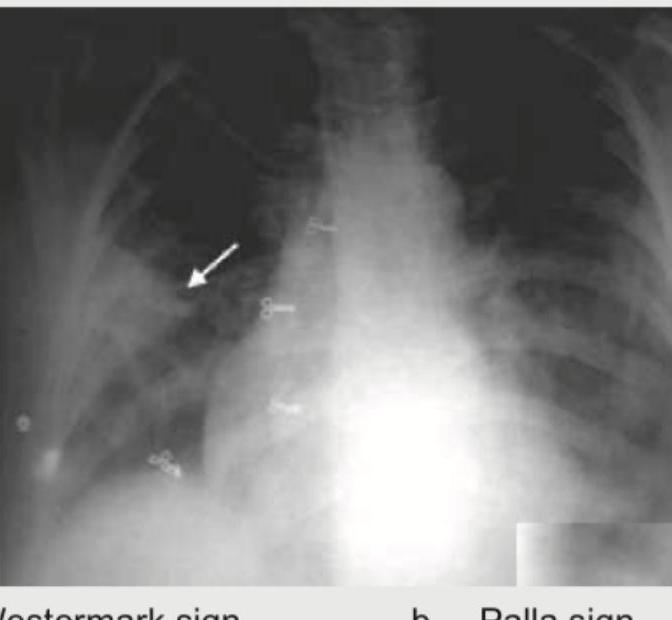
Which of the following is shown in the image below?
A 35-year-old lady presents with fever, skin rash and dyspnea on exertion for last 2 months. Her chest X-ray is shown below. What is the most likely diagnosis?

An AIDS patient presents with respiratory distress. CXR shows:

Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app