
Chest Radiology — MCQs

On this page
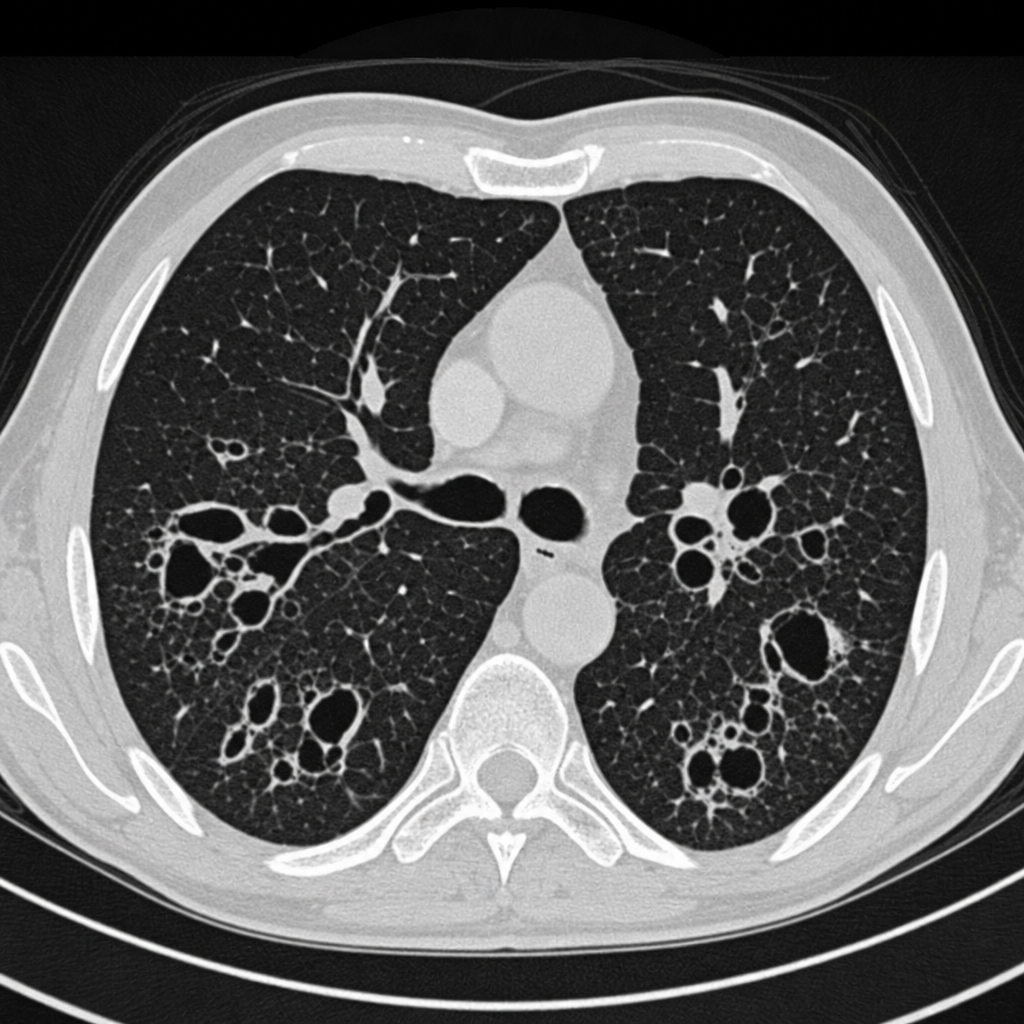
The CT chest of a patient shows the presence of what abnormality?
A 45-year-old male presents to the emergency department at 1 AM after binge drinking, complaining of severe chest pain following an episode of vomiting. A chest radiograph of this patient demonstrates which of the following signs?
Which one of the following diagnostic techniques is most specific for pulmonary embolism?
Consolidation of which part of the lung is likely to obliterate the aortic knuckle on a chest X-ray?
A 25-year-old man presented with fever, cough, expectoration, and breathlessness of 2 months' duration. Contrast-enhanced computed tomography of the chest showed bilateral upper lobe fibrotic lesions and mediastinal enlarged necrotic nodes with peripheral rim enhancement. Which one of the following is the most probable diagnosis?
Which of the following is NOT typically seen in congestive cardiac failure?
Pruned tree appearance of pulmonary circulation is a feature of which condition?
Which of the following conditions is best investigated with a non-contrast CT scan?
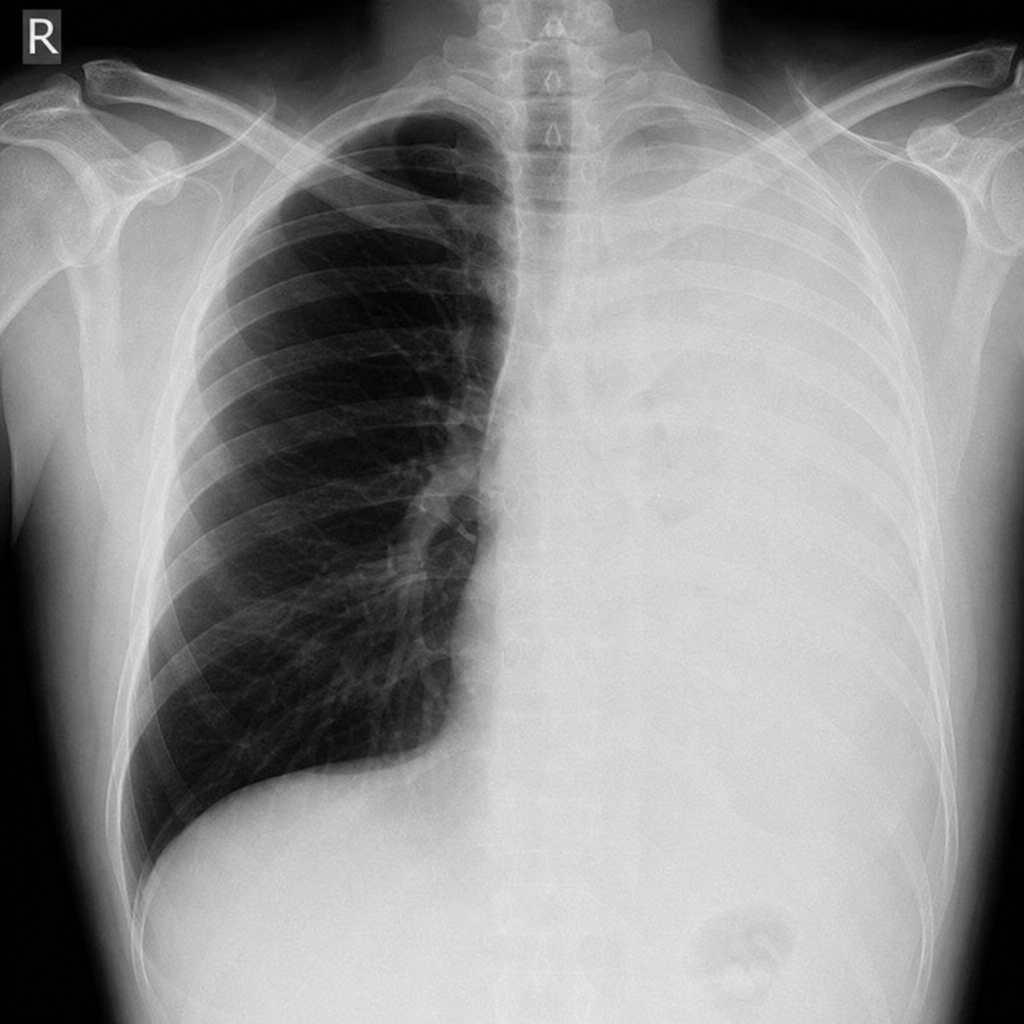
The following X-ray was taken after Staph. aureus pneumonia. What is the most likely complication?
A 45-year-old man presents with a 3-day history of breathlessness, fever, and dry cough. He recently traveled to China. Nasal and throat swabs have been collected, and a chest CT scan has been performed. Which of the following CT chest findings is most likely to be observed in this patient?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app