
Chest Radiology — MCQs

On this page
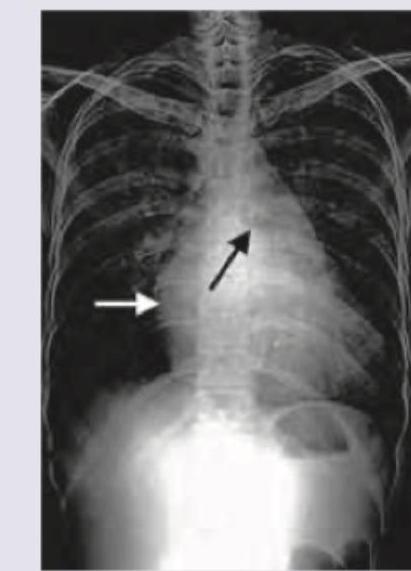
The CXR given shows presence of:

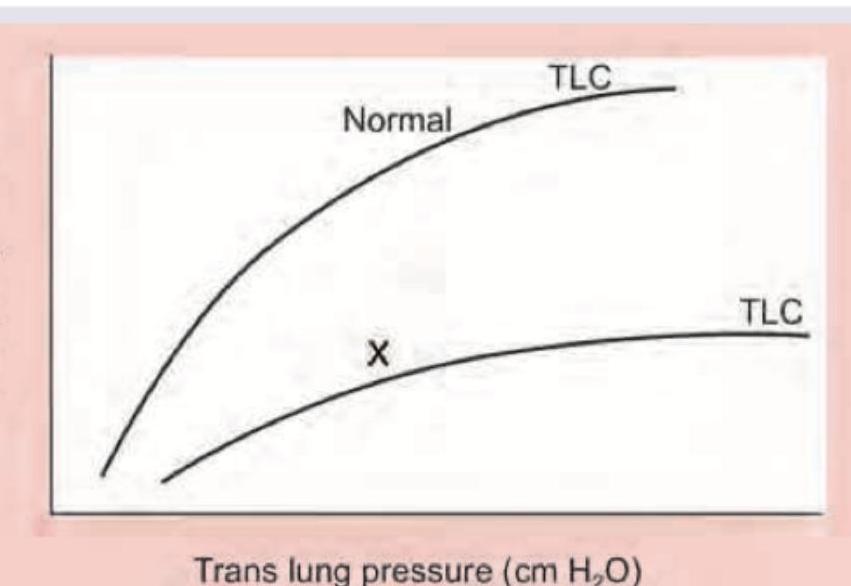
Which lung disease is shown in the image below marked as X?
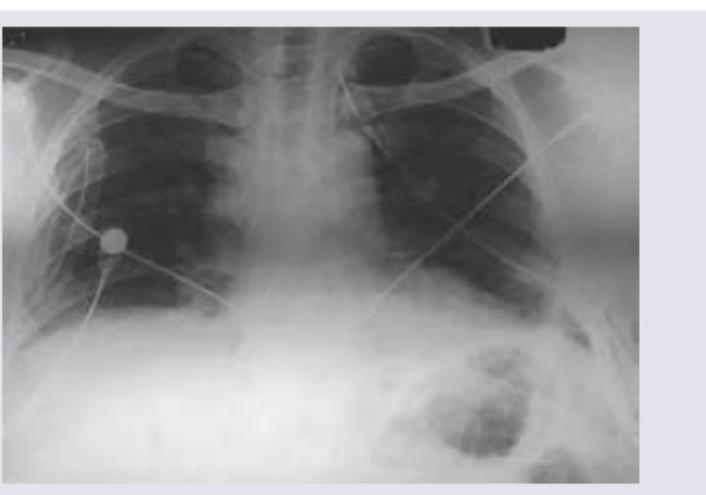
A 16-year-old boy is admitted with rapidly accumulating bilateral pleural effusion. His chest X-ray is shown below. Which of the following is incorrect about the X-ray shown?
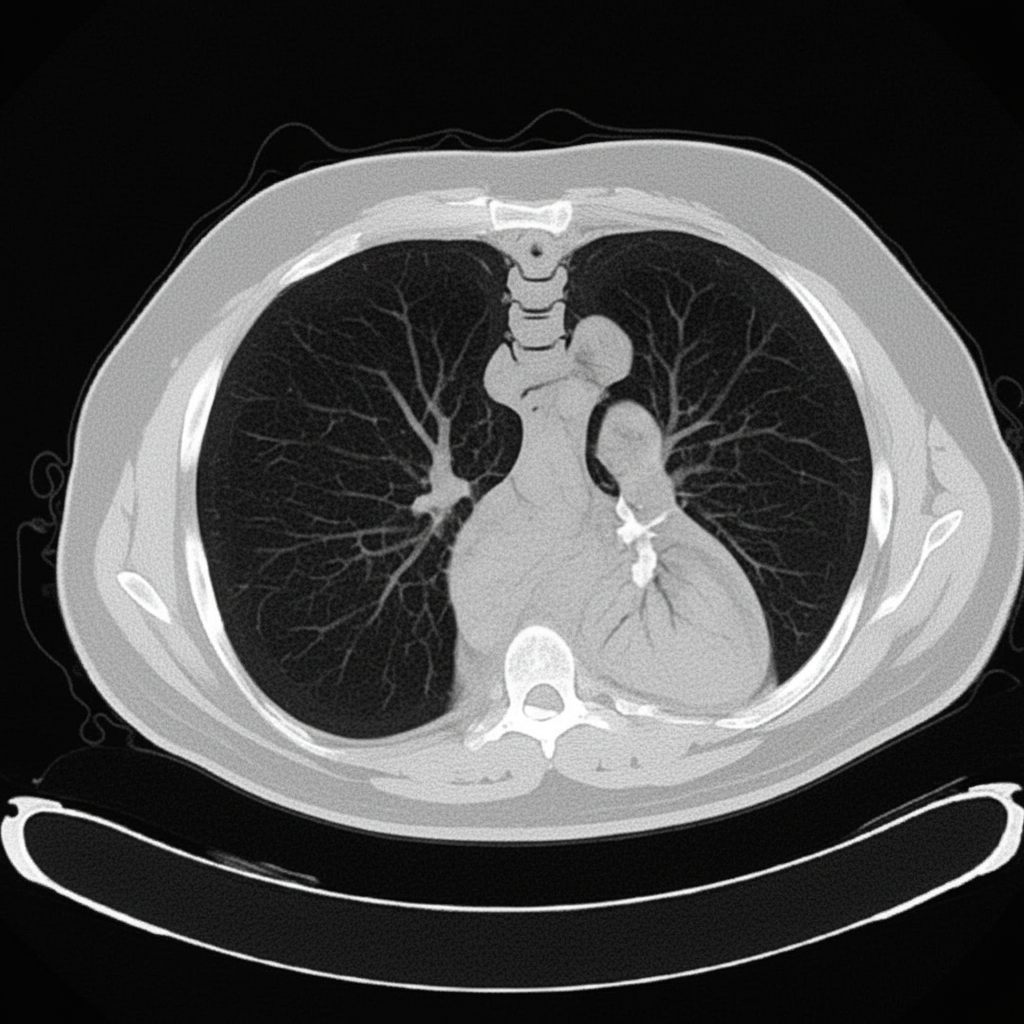
The CT chest shows presence of:
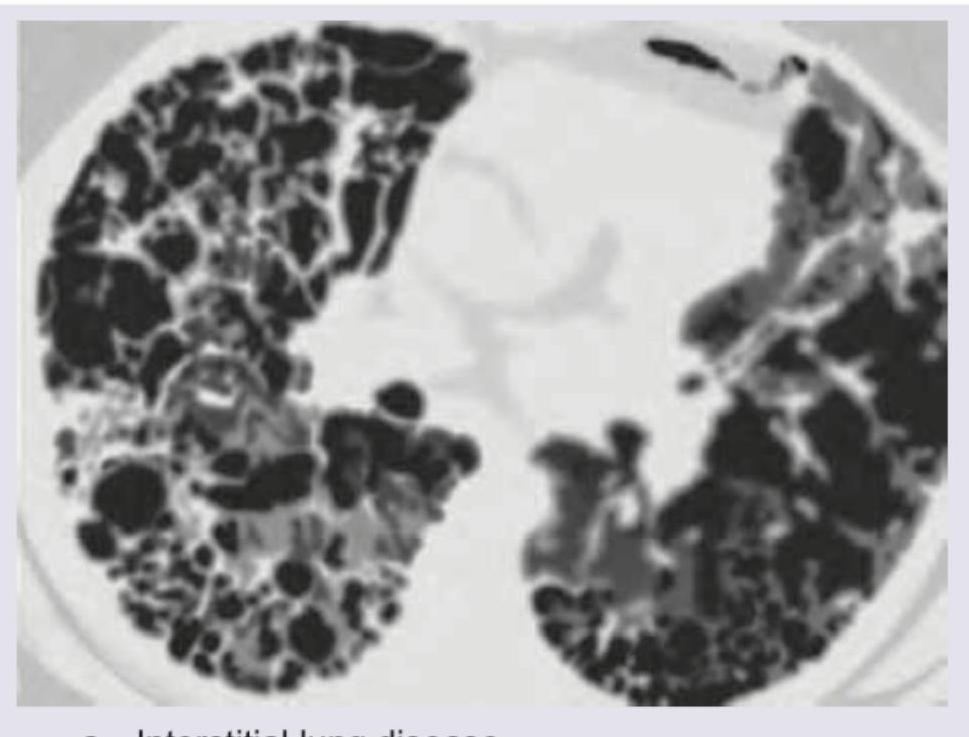
The image provided represents:
The image shows presence of:

The CT chest of a patient shows:

The CXR shows markings near the costophrenic angle. Which of the following is the cause of these markings? (Recent NEET Pattern 2016-17)

Chest X-ray was performed on a patient with malar flush and effort intolerance. All are true about the condition shown in the figure except:
A 65-year-old hypertension patient presents with chest pain, difficulty in breathing for 1 hour. Based on the chest X-ray shown below, identify the radiological finding:

Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app