
Chest Radiology — MCQs

On this page
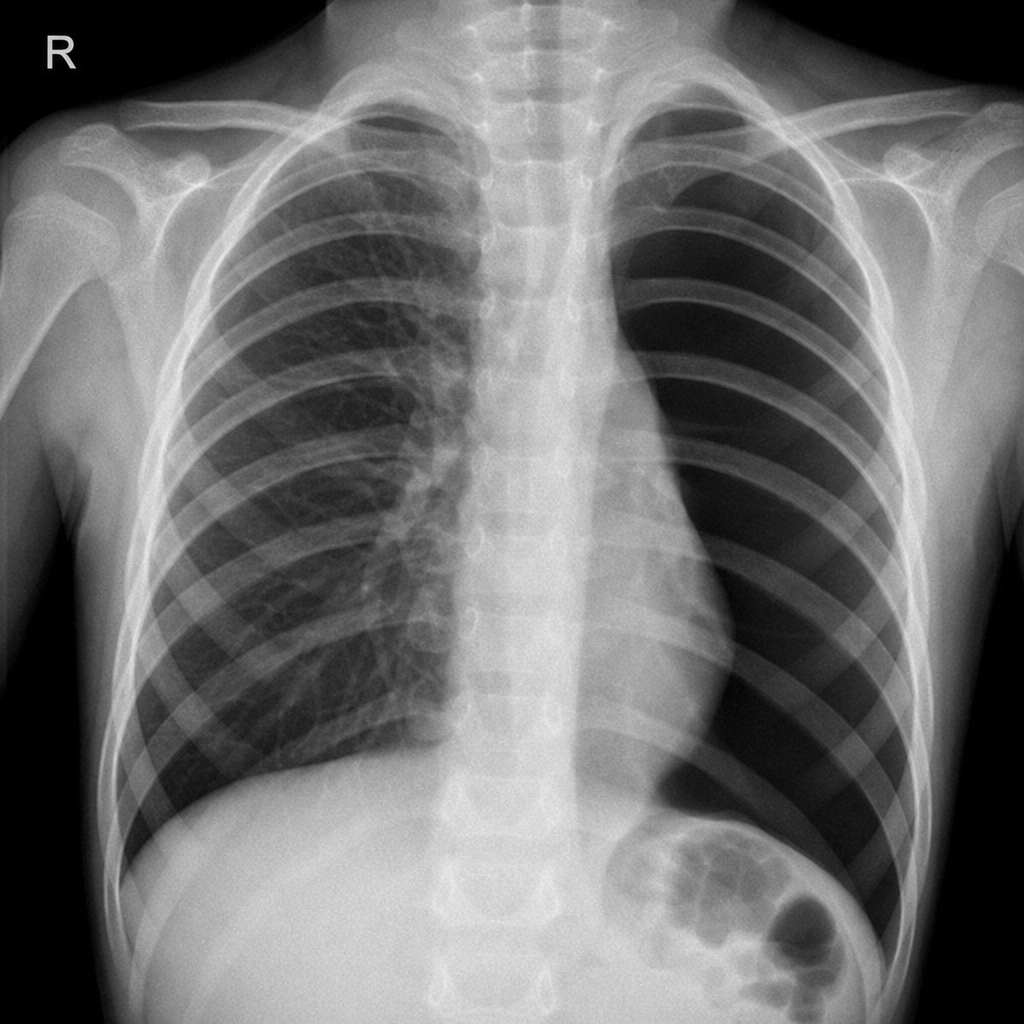
Chest x-ray of a child presenting with acute breathlessness. What is the most likely diagnosis?
What is the most common view used for a chest X-ray?
What is the investigation of choice for a Pancoast tumor?
The 'Floating Water Lily' sign is associated with which of the following conditions?
Round pneumonia is seen with
Finger-in-glove sign is seen in
Based on the provided chest X-ray image of a patient presenting with low-grade fever, which infection is most likely?

On CT chest, the 'halo sign' is particularly associated with which condition in immunocompromised patients?
Which condition is characterized by a specific appearance on CT scans that resembles small centrilobular nodules with branching linear structures?
Air bronchogram on chest X-ray denotes -
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app