
Chest Radiology — MCQs

On this page
Which of the following radiographic features is most characteristically associated with the pathophysiology of congestive heart failure?
In a patient with a suspected mediastinal mass, which imaging modality is most appropriate for initial evaluation?
Identify the most likely diagnosis based on the chest X-ray findings in a patient with low-grade fever.
Which radiographic sign is most characteristic of acute alveolar pulmonary edema?
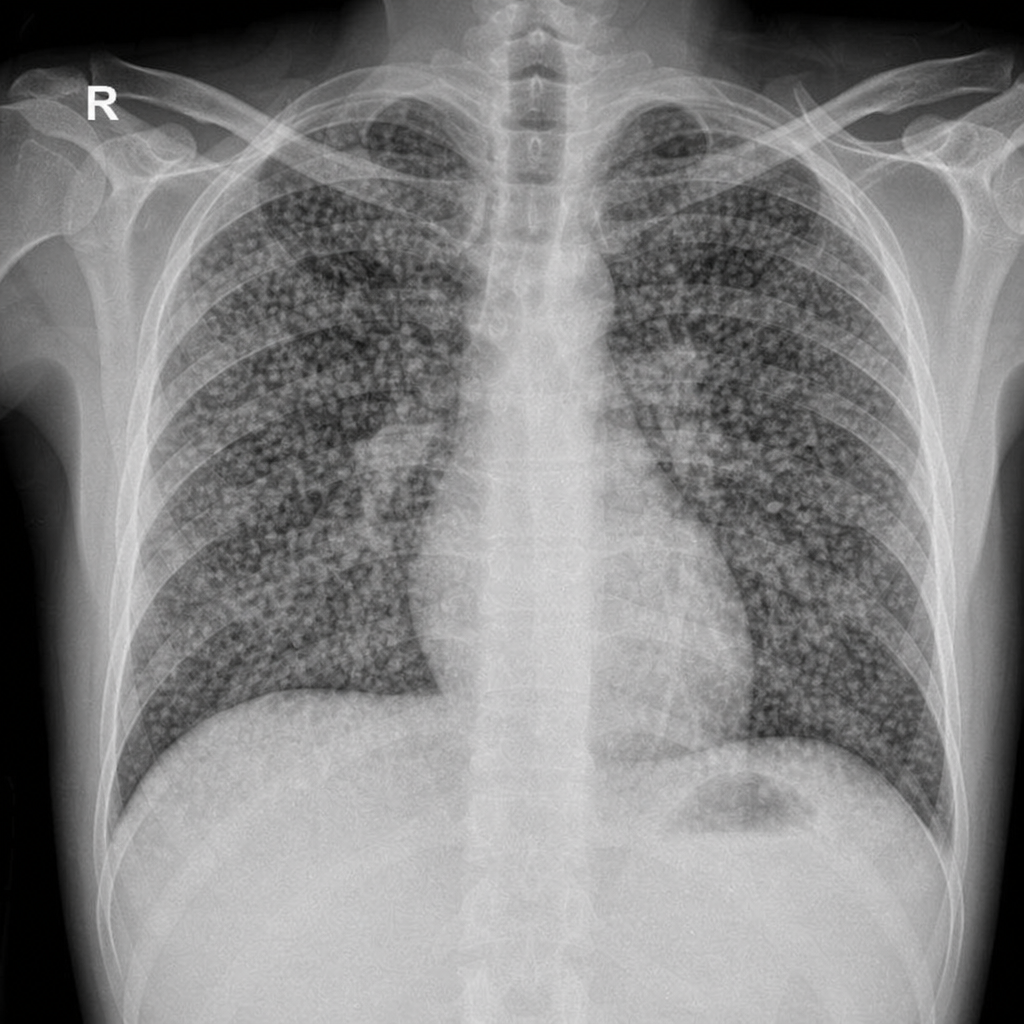
Snow storm appearance on chest X-ray is seen in -
Identify the condition represented in the chest radiograph.

Kerley B lines are seen in mitral stenosis when the resting left atrial pressure exceeds which value?
Which of the following is NOT a chest radiographic feature of left atrial enlargement?
HRCT features of interstitial pneumonia include all of the following EXCEPT:
Which of the following statements about HRCT (High Resolution Computed Tomography) is false?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app