
Chest Radiology — MCQs

On this page
A CT pulmonary angiogram shows intravascular webs and bands. Which additional finding would best support chronic pulmonary embolism?
A lung biopsy shows 'temporal heterogeneity' with fibroblastic foci. Which radiological pattern would best support usual interstitial pneumonia?
A chest X-ray shows a 'silhouette sign' with opacity obscuring the right heart border. Which lobe of the lung is most likely affected?
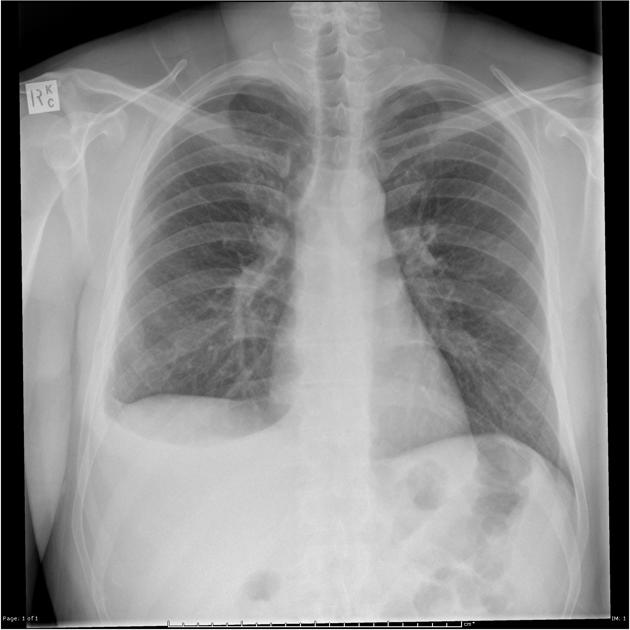
PA view of chest X-ray is given here. What is the diagnosis?

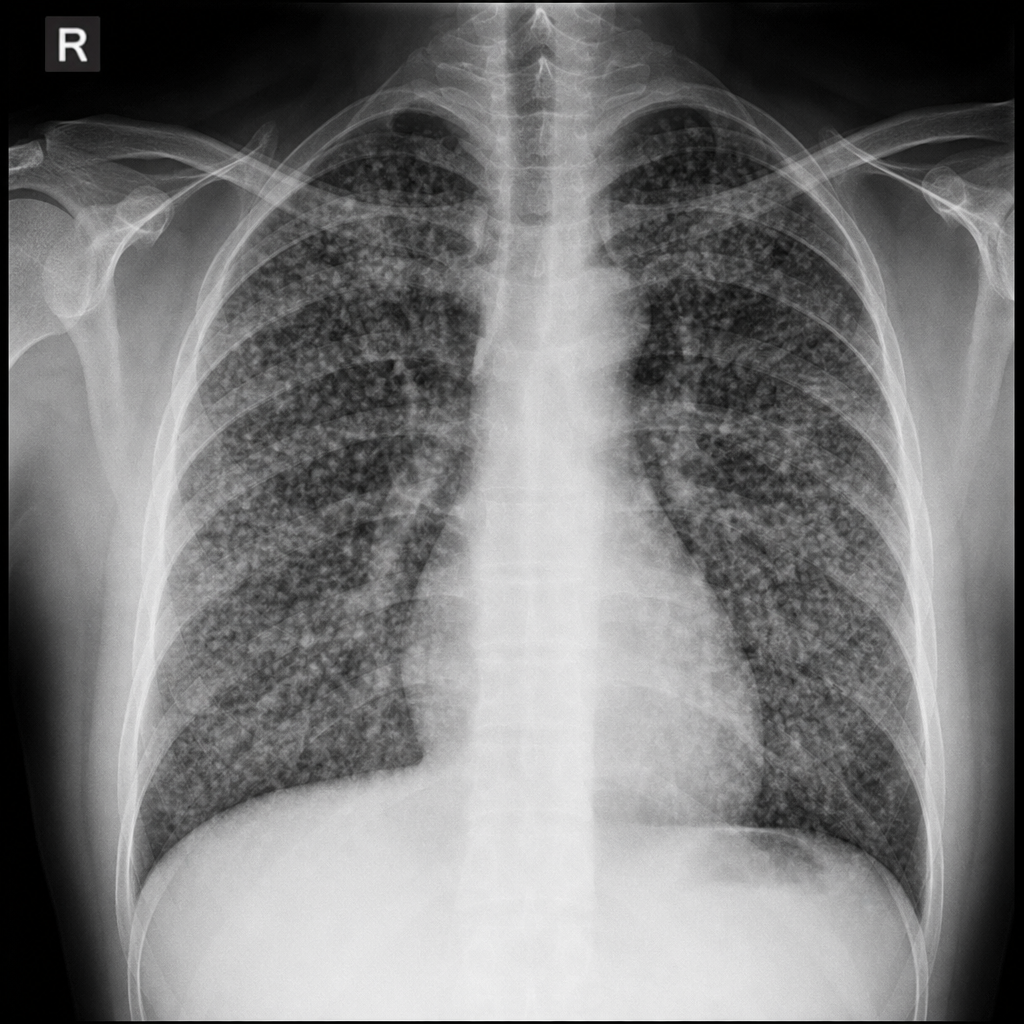
A patient presented with complaints of dyspnoea. The shown X-ray is suggestive of:
Left cardiac border bulge can be seen in all, except -
A 10yr old boy with a known case of nephrotic syndrome since 4 years on treatment brought to the pediatric OPD with chief complaint of difficulty in breathing. There is no history of fever. On examination, respiratory system was normal except slightly reduced breath sounds on right infra-axillary region. Paediatrician thinks of pleural effusion. What is next best modality of investigation to detect pleural effusion?
A patient of RTA with injury over chest and limbs has low SpO2. M-mode ultrasound of right upper chest shows stratosphere sign. What is the diagnosis?
X-ray given below suggests:
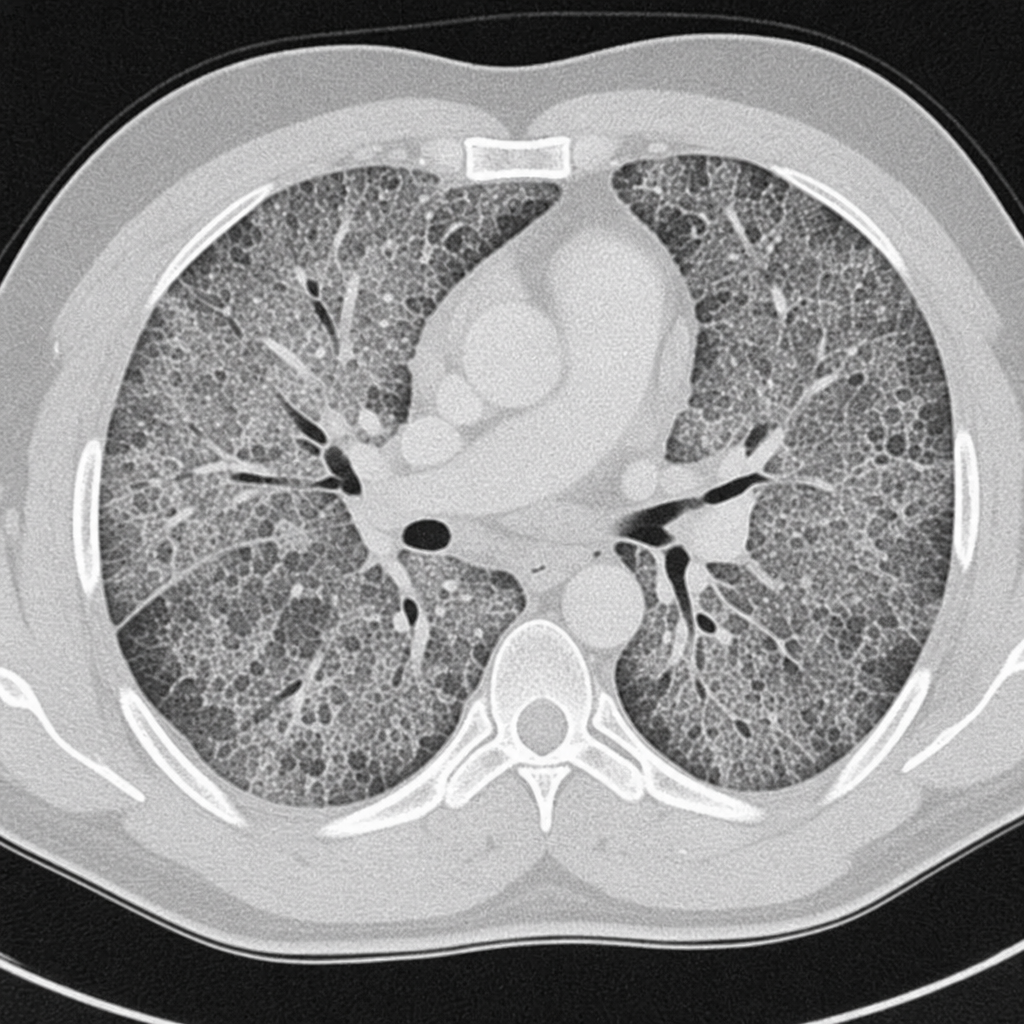
Chest CT shows bilateral ground-glass opacities with crazy paving pattern and preserved bronchial markings. Likely diagnosis?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app