
Chest Radiology — MCQs

On this page
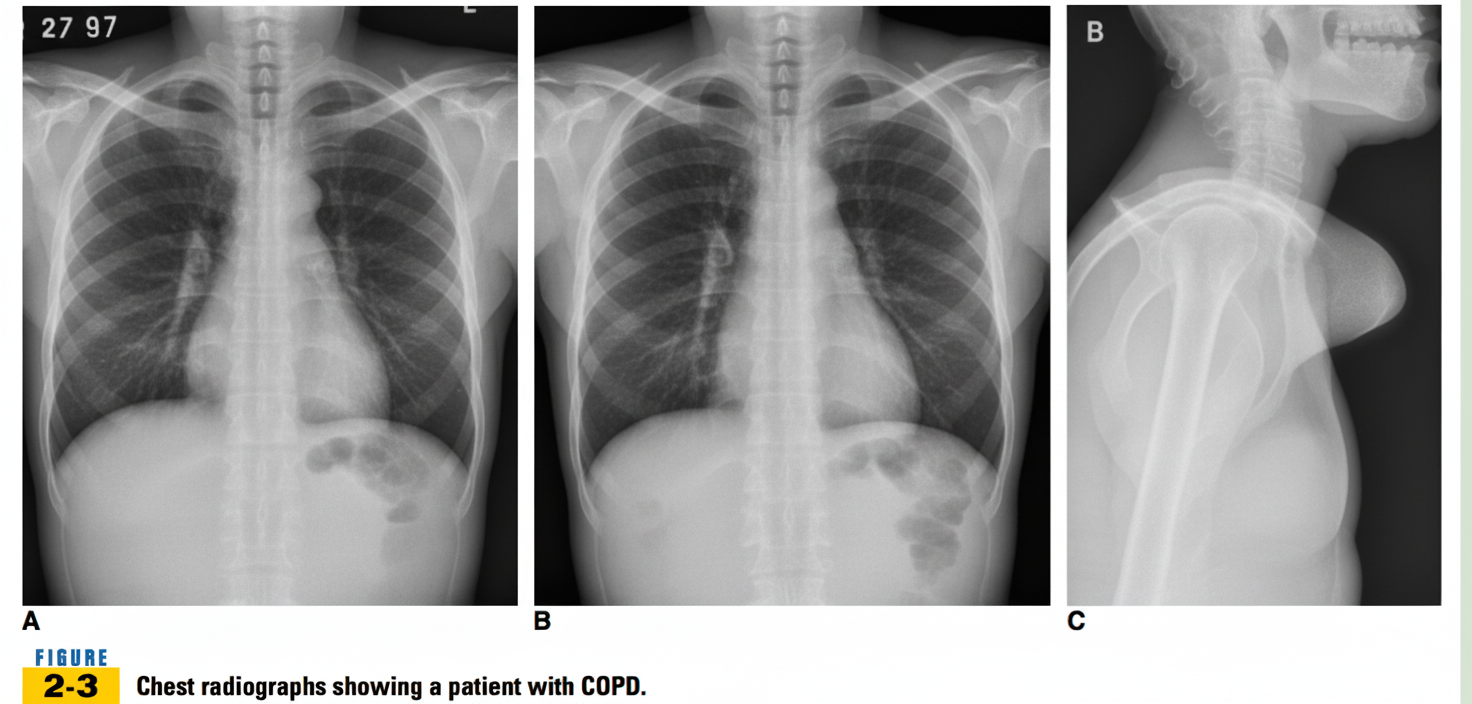
Based on the provided image, what is the most likely diagnosis?
What is the most helpful radiological investigation in a patient suspected of left pleural effusion?
The "sandstorm" appearance on a chest radiograph is characteristic of which condition?
High-resolution CT of the lung is a specialized CT technique that utilizes what to provide greater detail of lung parenchyma?
The 'Comet Tail Sign' is most characteristically seen in which of the following conditions?
Which of the following is a cause of a unilateral hyperlucent lung on chest radiography?
Egg shell calcification is seen in which of the following conditions?
Which of the following radiological findings does NOT indicate increased pulmonary blood flow?
What is the cause of an opaque hemithorax?
An expiratory chest radiograph is particularly useful to detect which of the following conditions?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app