
Chest Radiology — MCQs

On this page
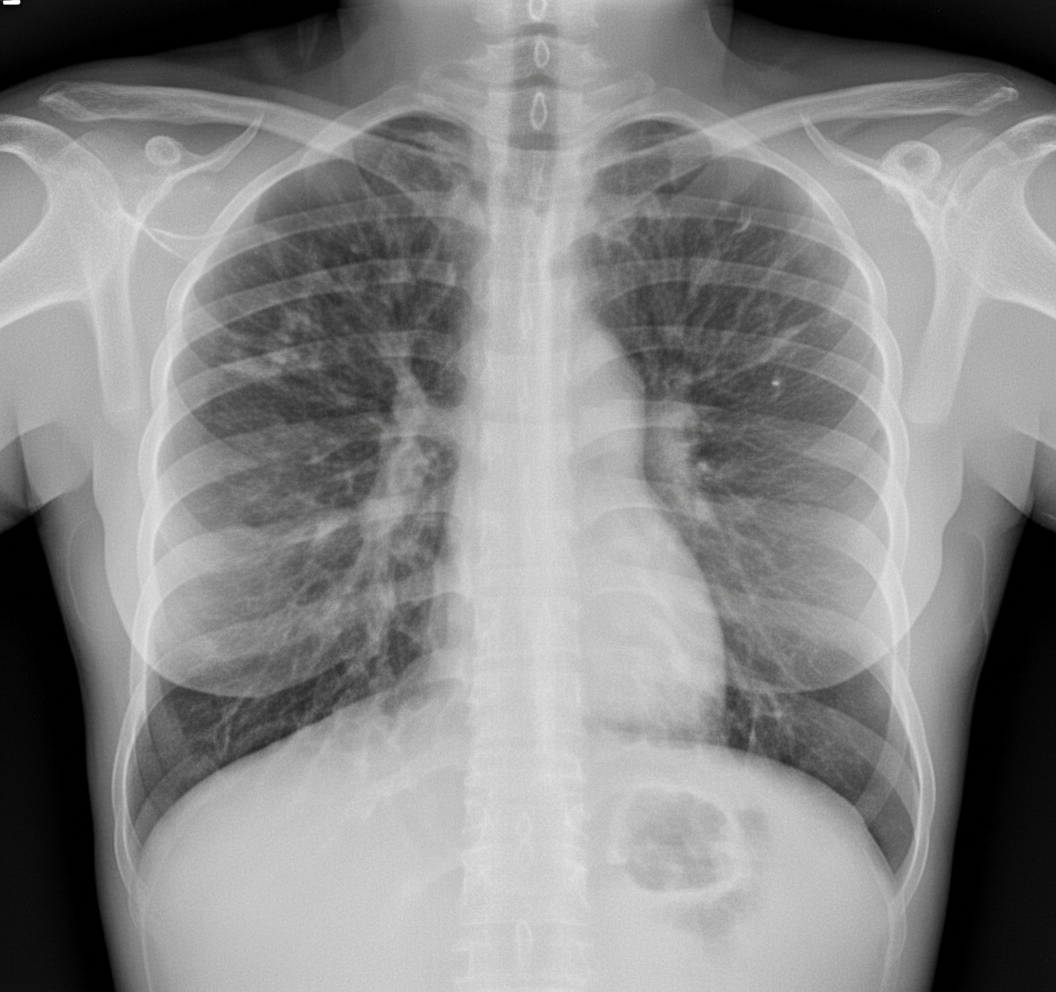
What does the CXR of a patient with cystic fibrosis show?
What does this CT chest image show?
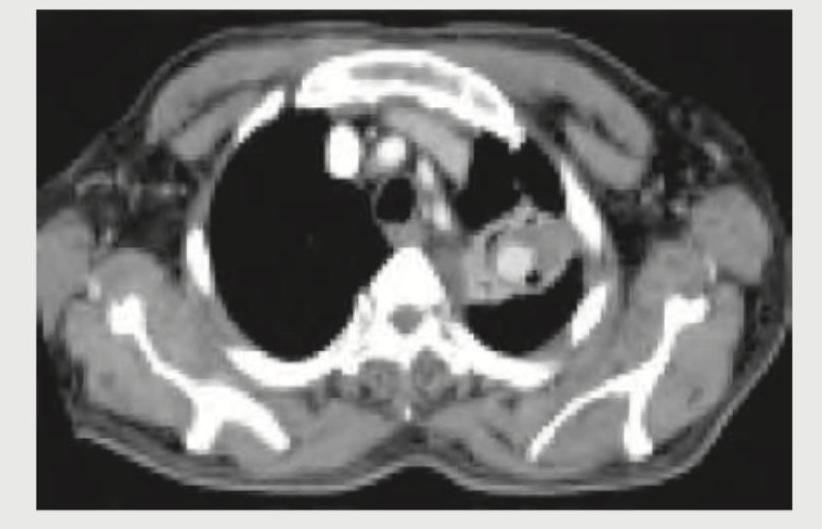
The given contrast enhanced CT scan chest shows presence of:
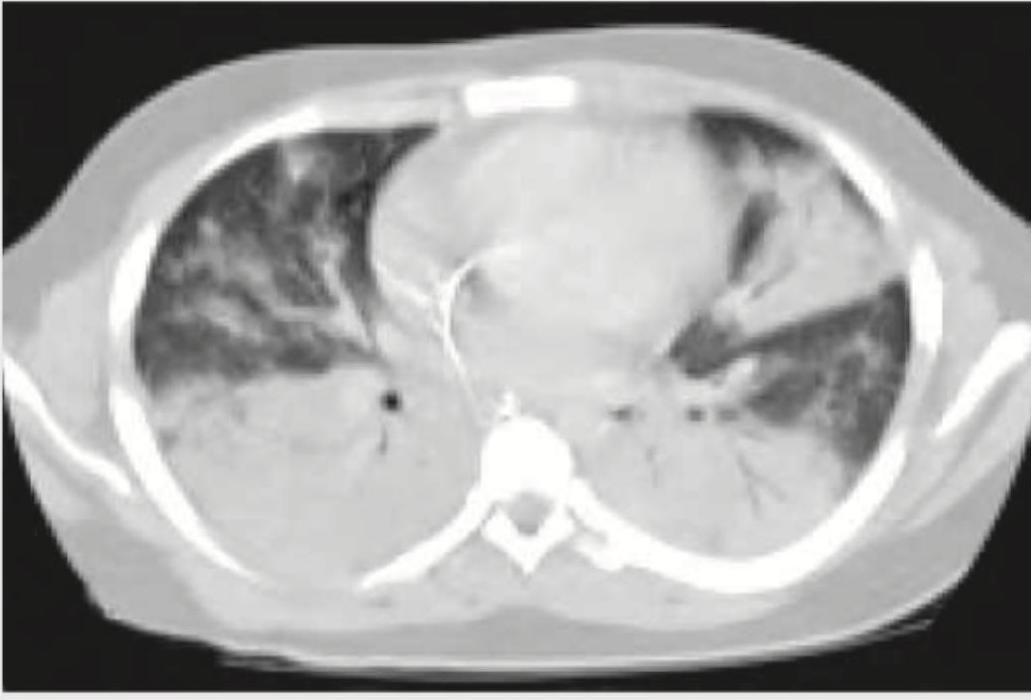
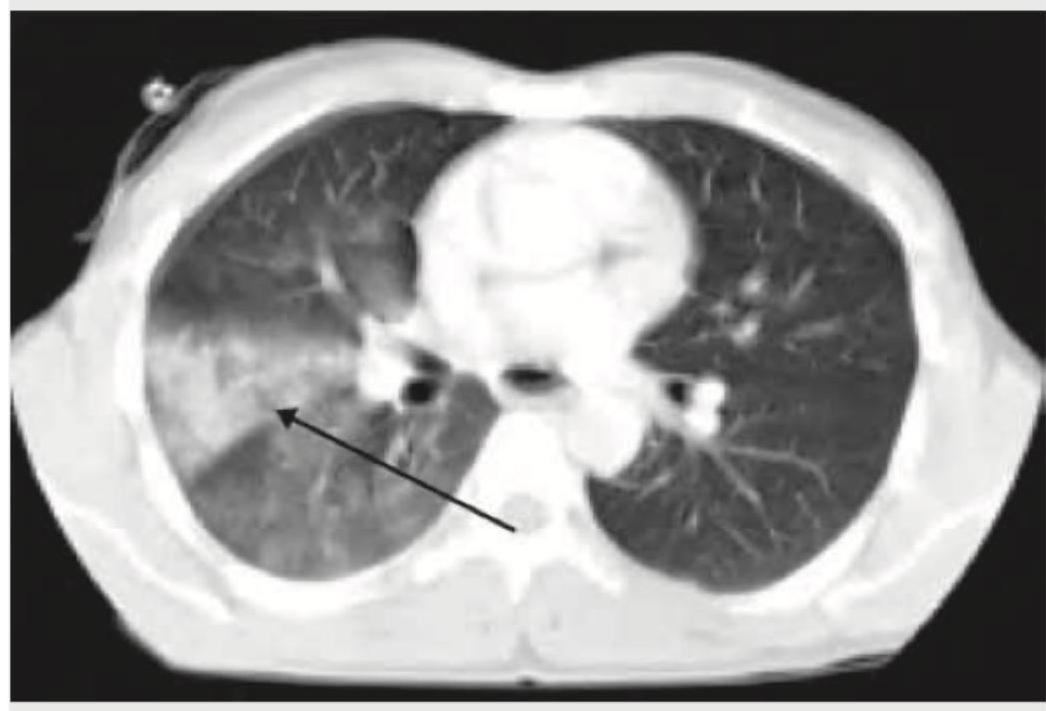
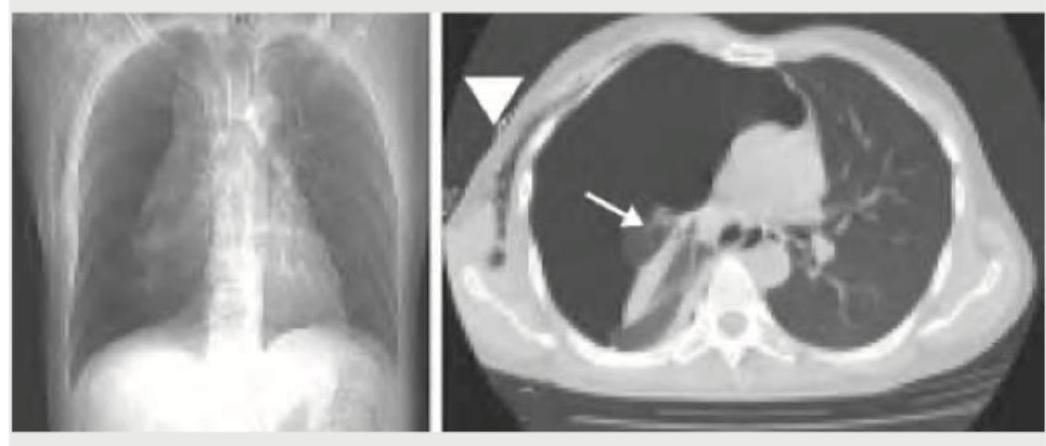
A cement slab fell on the chest of a 20-year-old construction worker. His condition deteriorated over the next 24 hours after admission, with acute hypoxemia and bilateral opacities not explained by cardiac failure or fluid overload. A repeat CT chest was performed. What does it show?
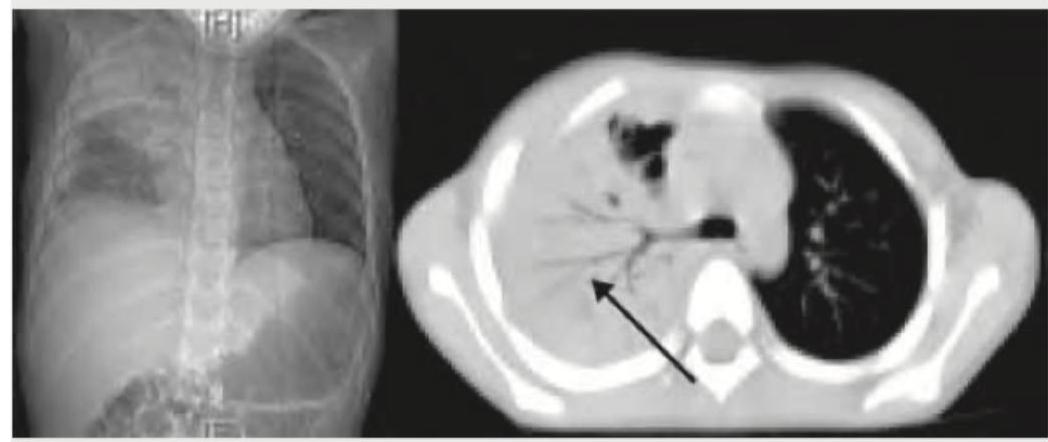
A cement slab fell on the chest of a 20-year-old construction worker. The arrow in the given CT chest points to:
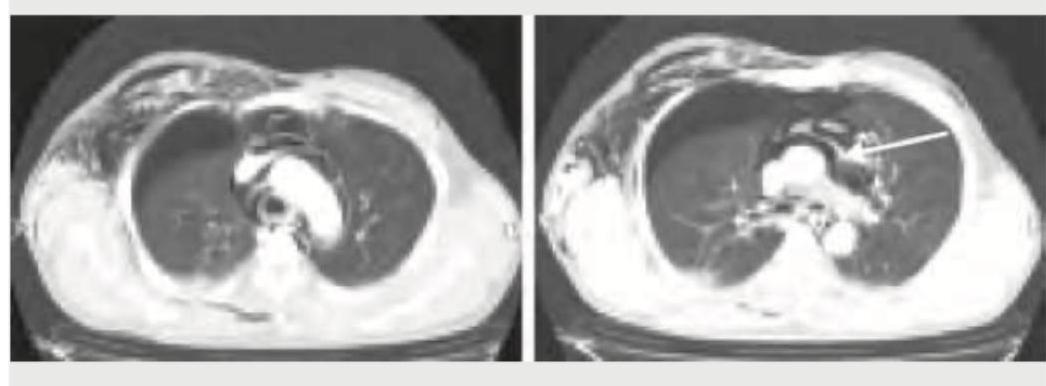
The arrow in the given CT chest points to:
What does the following CT chest show?
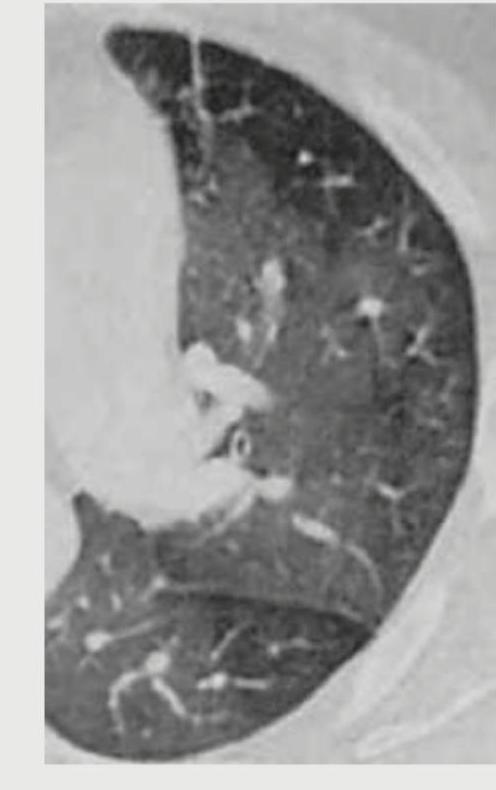
The following lung window in CT chest is taken in which phase of respiration?

The lung parenchyma on CT chest shown below is best described as:
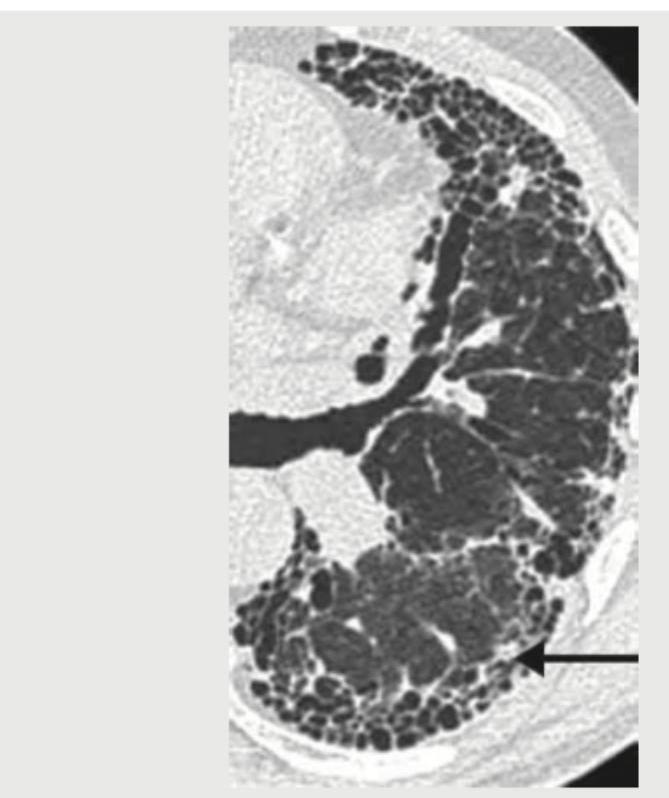
An 18-year-old boy is brought to the hospital with difficulty in breathing after a bar fight. What does the given CT chest show?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app