
Chest Radiology — MCQs

On this page
The image shows a standing upright chest X-ray with pleural reflection and a straight horizontal air-fluid level with absence of meniscus sign. What is the most likely diagnosis?

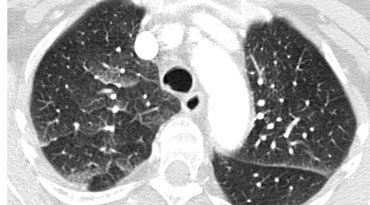
The CT chest image shows a hazy increased attenuation with preserved bronchial and vascular markings. What pattern is demonstrated?
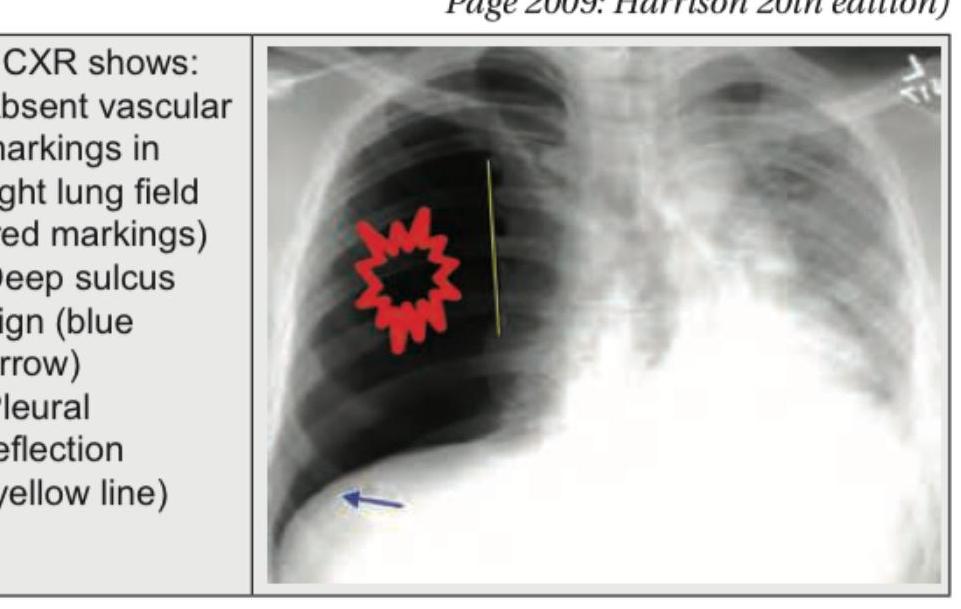
A 45-year-old male presents with sudden onset shortness of breath and chest pain. A chest X-ray is obtained. What is the most likely diagnosis based on the image?
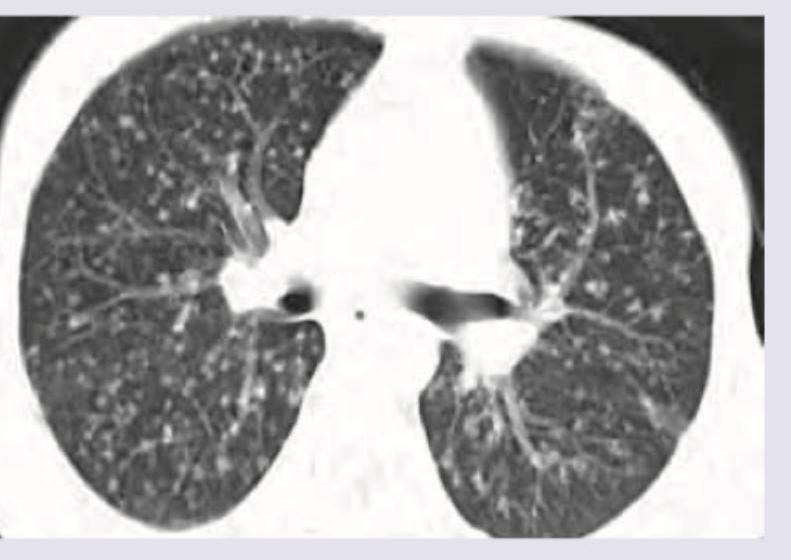
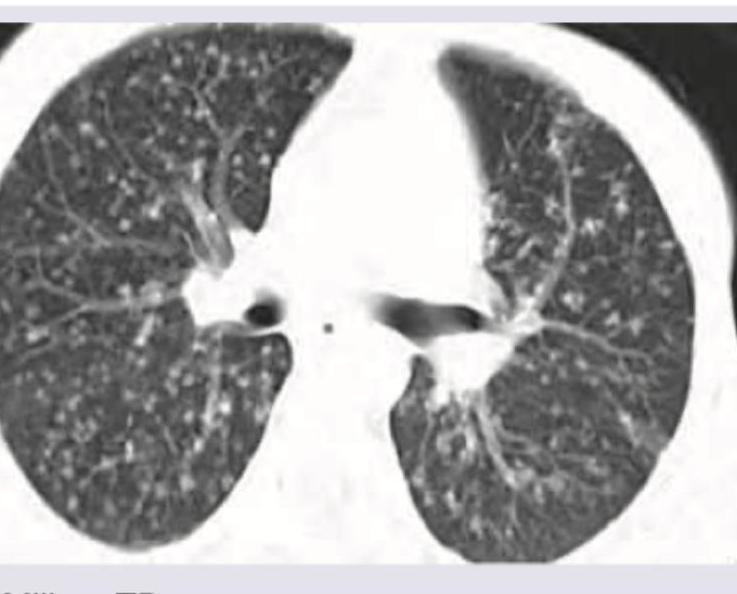
The following pattern in CT scan shown below can occur due to spread from:
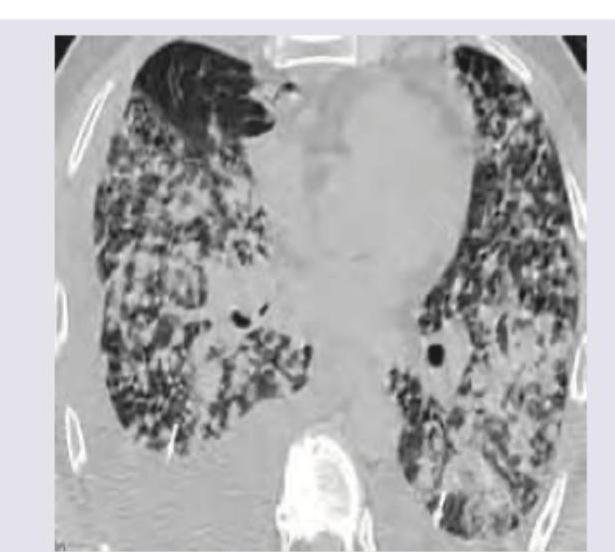
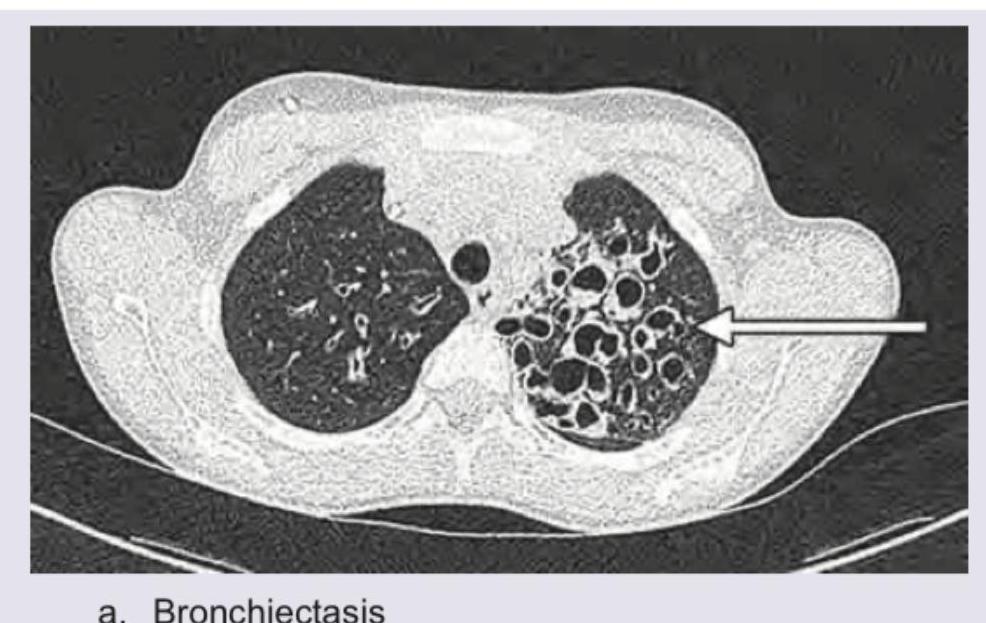
The following CT chest shows presence of:
A 35-year-old male presents with fever, night sweats, and weight loss for 6 weeks. He has a history of close contact with a known TB patient. The given CT scan chest shows presence of:
The CT chest of a patient given below shows presence of: (Recent NEET Pattern 2016-17)
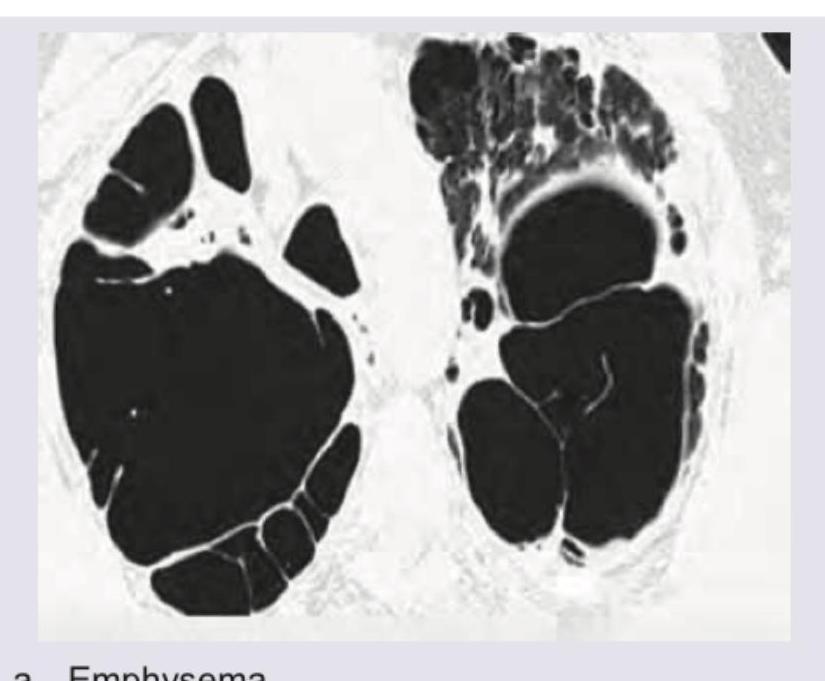
The following CT chest shows presence of:
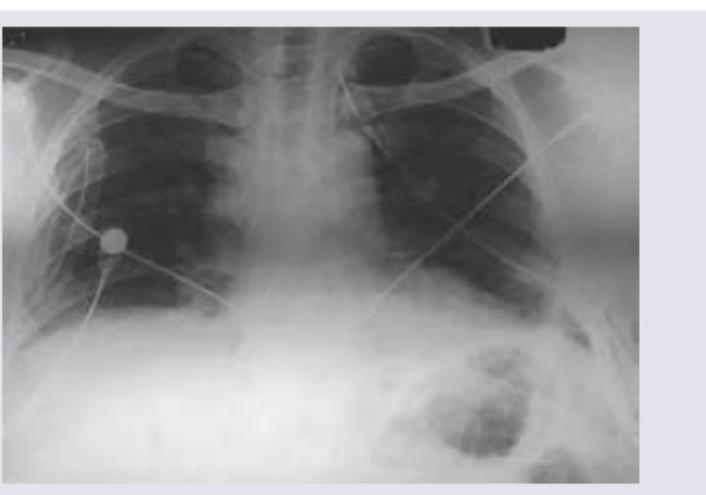
The CXR given shows presence of:

A 16-year-old boy is admitted with rapidly accumulating bilateral pleural effusion. His chest X-ray is shown below. Which of the following is incorrect about the X-ray shown?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app