
Chest Radiology — MCQs

On this page
Nipple shadows in a chest X-ray characteristically have a sharp:
Minimum fluid collection required for radiological detection of pleural effusion in lateral decubitus view is:
A young man with tuberculosis presents with massive recurrent hemoptysis. What is the most probable cause?
What is the most reliable method for diagnosing pulmonary embolism?
Which of the following is NOT a radiographic finding of Congestive Heart Failure (CHF)?
A patient presents with bilateral hilar lymphadenopathy with eggshell calcification on chest X-ray. What is the most likely diagnosis?
A patient with a history of occupational asbestos exposure presents with SOB and fatigue. CXR was done. What is the diagnosis? 
Based on the provided chest X-ray images, what is the most likely diagnosis?
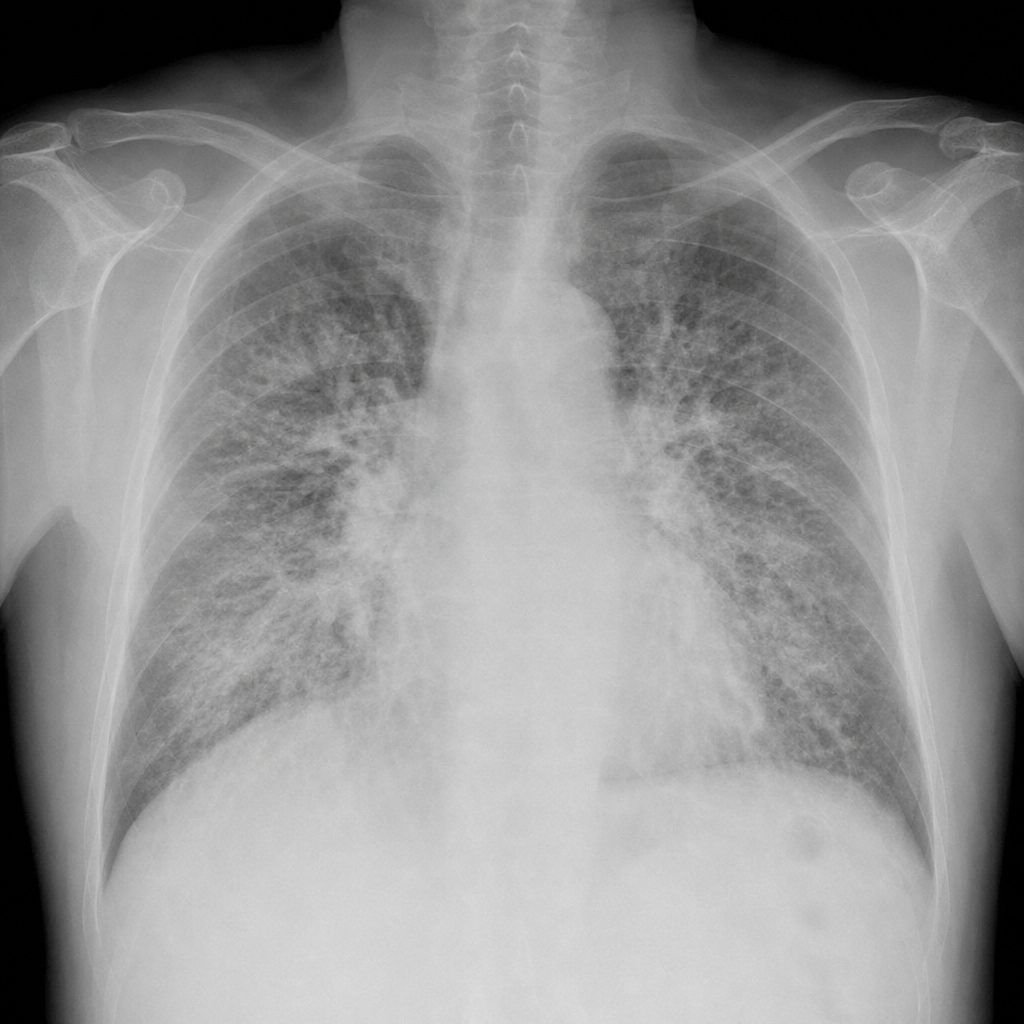
A chest X-ray is shown below. What is the most likely diagnosis?
A patient with a history of breast cancer underwent Cobalt-60 radiotherapy involving the right thorax. She now presents with respiratory distress 1–6 months after completing radiotherapy, and imaging shows haziness in the right lung that is sharply demarcated and conforms to the radiation field. What is the most likely diagnosis?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app