
Chest Radiology — MCQs

On this page
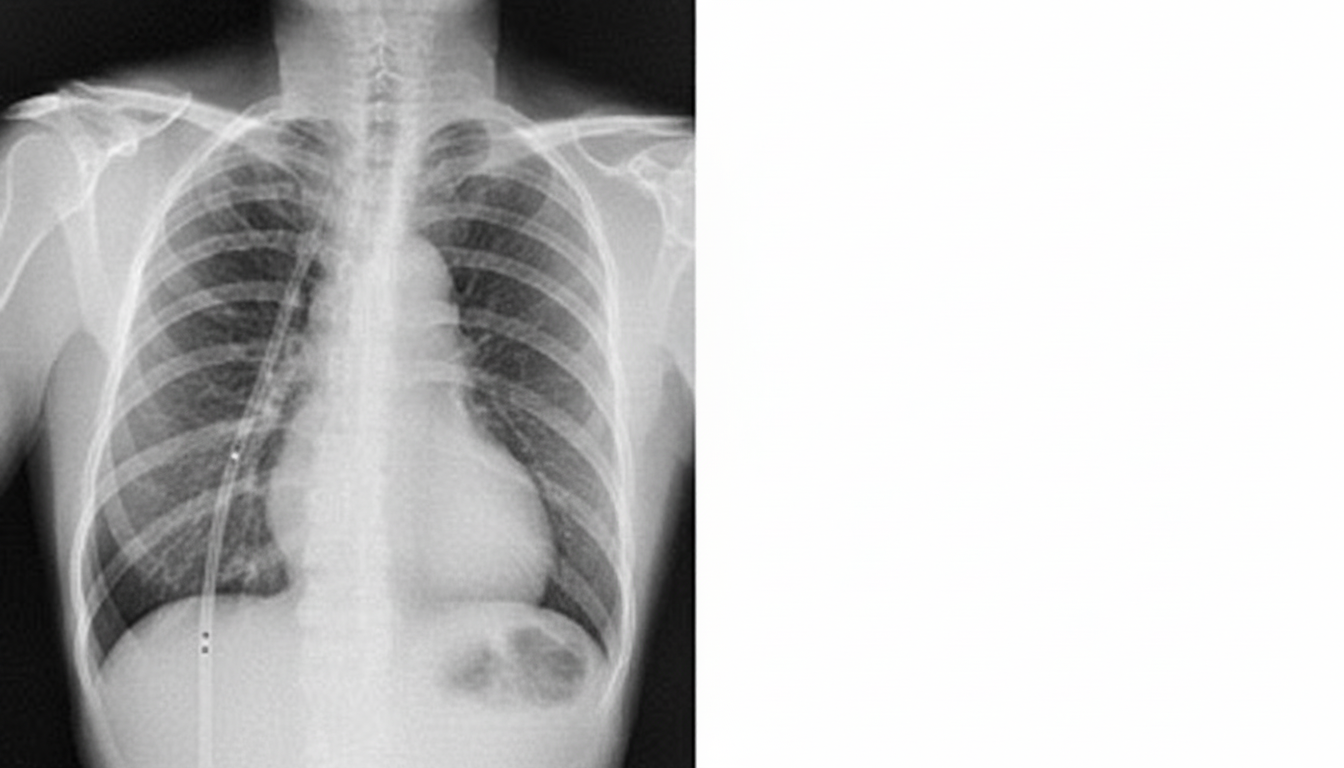
The tube visible in the chest X-ray below is located in which anatomical space?
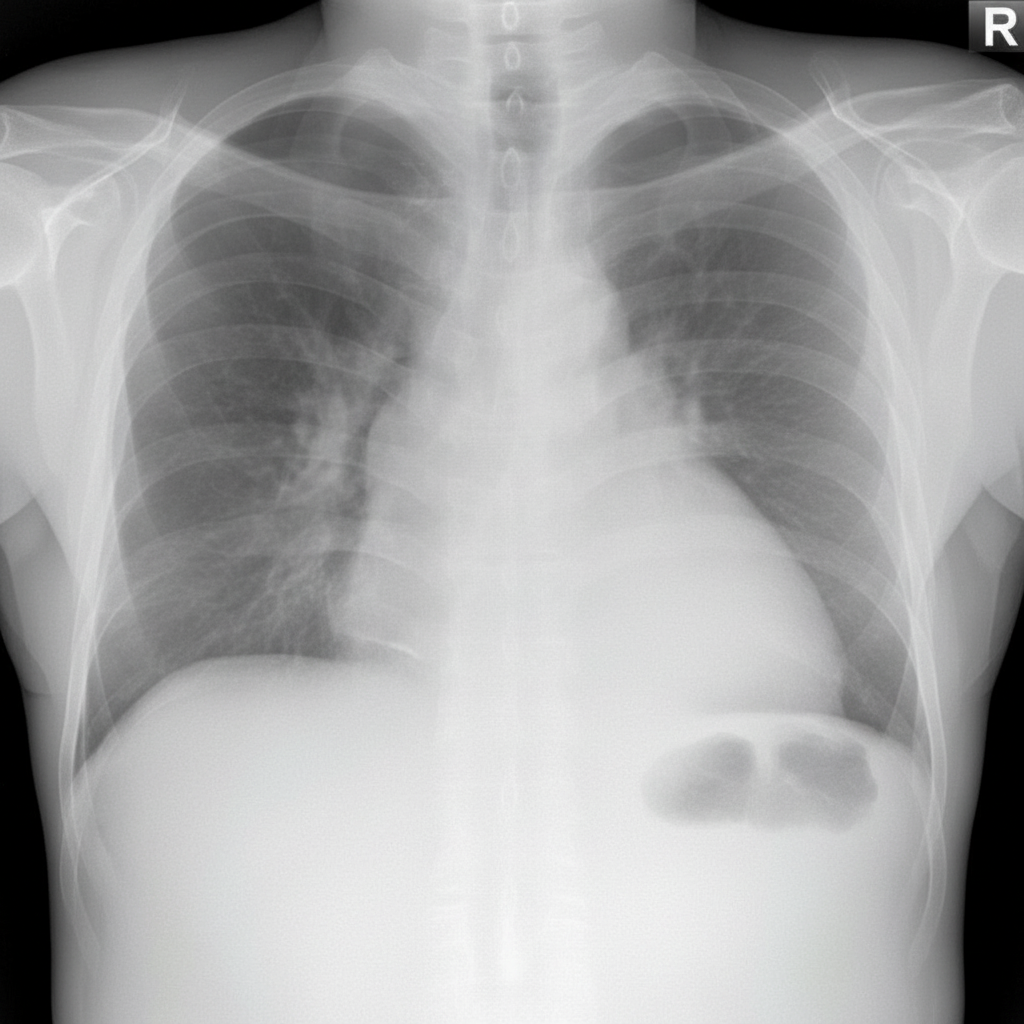
A 53-year-old female nonsmoker is being evaluated with symptoms of progressive shortness of breath. She has a past history of trauma to the right side of the chest. There is no history of asthma, sputum production, or recent chest pain. Chest X-ray is shown. What is the likely diagnosis?
HRCT is the investigation of choice for diagnosing all of the following conditions, EXCEPT?
Kerley B lines are seen in which of the following conditions?
Which of the following statements is NOT true regarding Pectus excavatum?
Superior rib notching is not associated with which of the enlisted conditions?
Pulmonary plethora is seen in which of the following conditions?
Westermark's sign is seen in which of the following conditions?
A chest X-ray shows an opacity in the lung with irregular calcification. What is this suggestive of?
Sequestration lung is best diagnosed by which imaging modality?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app