
Chest Radiology — MCQs

On this page
Which of the following features is characteristic of a benign lung lesion?
Which sign on chest X-ray is suggestive of carcinoma lung?
Which of the following radiological signs is typically present in a patient with symptoms suggestive of pulmonary embolism?
What is an early radiographic sign of pulmonary edema on a chest X-ray?
What volume of fluid is required to produce costophrenic angle blunting on erect chest X-ray in cases of pleural effusion?
Rib notching is a characteristic radiological finding in which of the following conditions?
If the right cardiac silhouette is obliterated, it means the pathology involves which of the following?
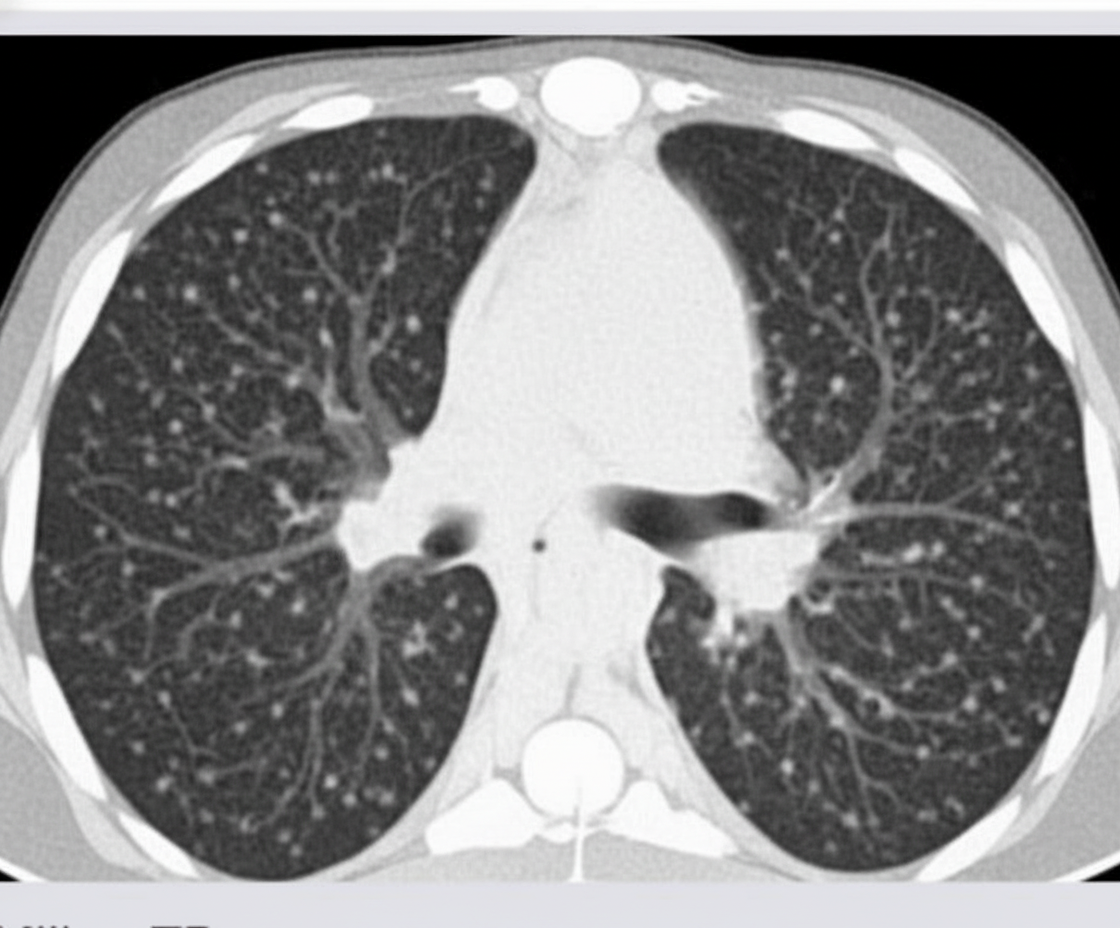
All are differential diagnoses for the CT chest finding shown, except?
Which of the following conditions characteristically show honeycomb lung on chest X-ray?
Bilateral pleural thickening in the lower and middle lung zones is a radiological feature of which condition?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app