
Chest Radiology — MCQs

On this page
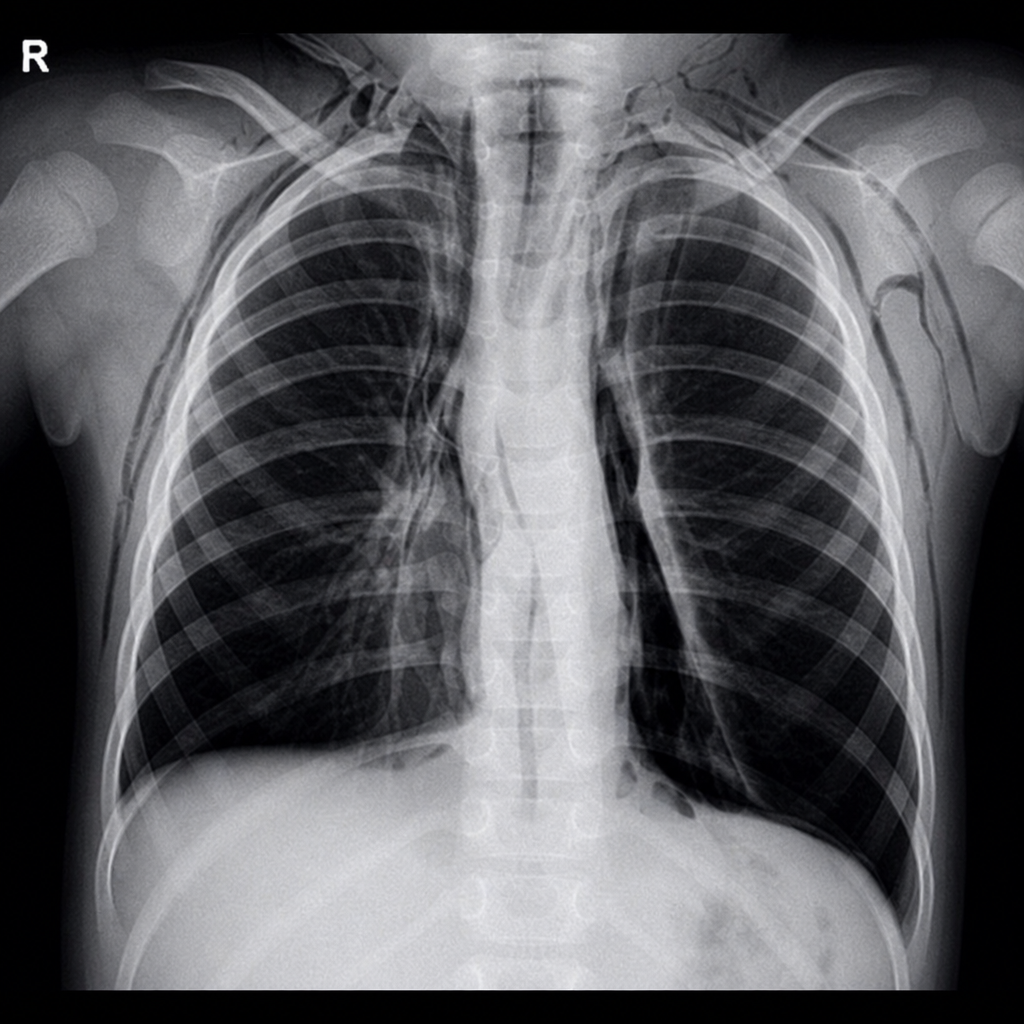
What is the diagnosis on chest X-ray?
Pulmonary embolism is best diagnosed by which imaging modality?
Which of the following statements regarding signs of pulmonary embolism are TRUE or FALSE?
Westermark sign is seen in which condition?
Mounier-Kuhn syndrome is characterized on imaging by which finding?
All of the following statements about Pneumococcal Pneumonia are true, except?
What is the earliest chest X-ray finding in cystic fibrosis?
Obliteration of the right cardiac silhouette on a chest X-ray suggests pathology involving which of the following structures?
A chest X-ray shows a homogenous opacity on the right side with a shift of the mediastinum to the opposite side. What is the most probable diagnosis?
What is the earliest feature of pulmonary venous hypertension?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app