
Chest Radiology — MCQs

On this page
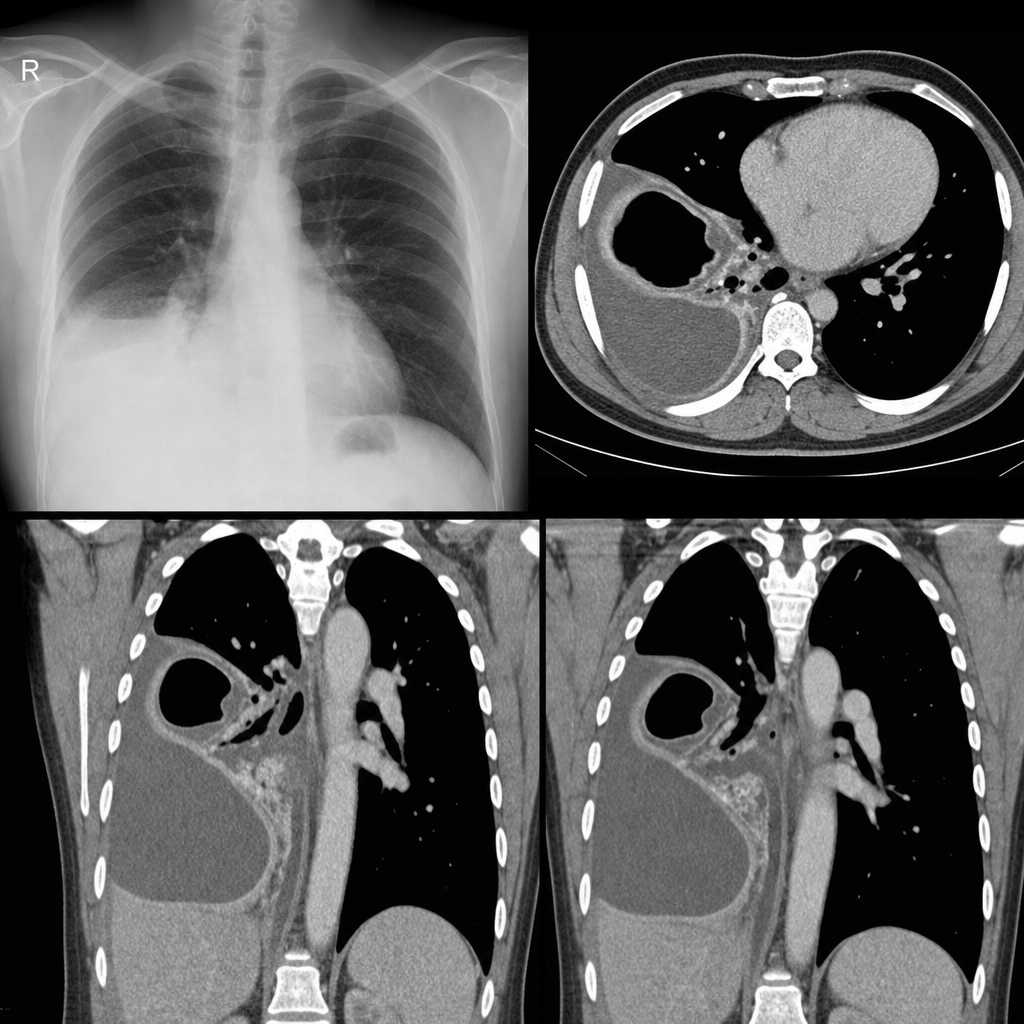
A 30-year-old male presents with a 3-week history of right-sided chest pain and cough. Examination reveals decreased breath sounds in the right lower lung. Chest X-ray shows blunting of the costophrenic angles. A contrast-enhanced CT scan of the chest is performed. What is the most probable diagnosis?
What is the investigation of choice for pleural effusion?
Kerley B lines are seen in which of the following conditions?
What is the investigation of choice for evaluating pleural diseases?
Which of the following chest x-ray findings is a common feature of ARDS and cardiogenic pulmonary edema?
What is the investigation of choice for the detection and characterization of interstitial lung disease?
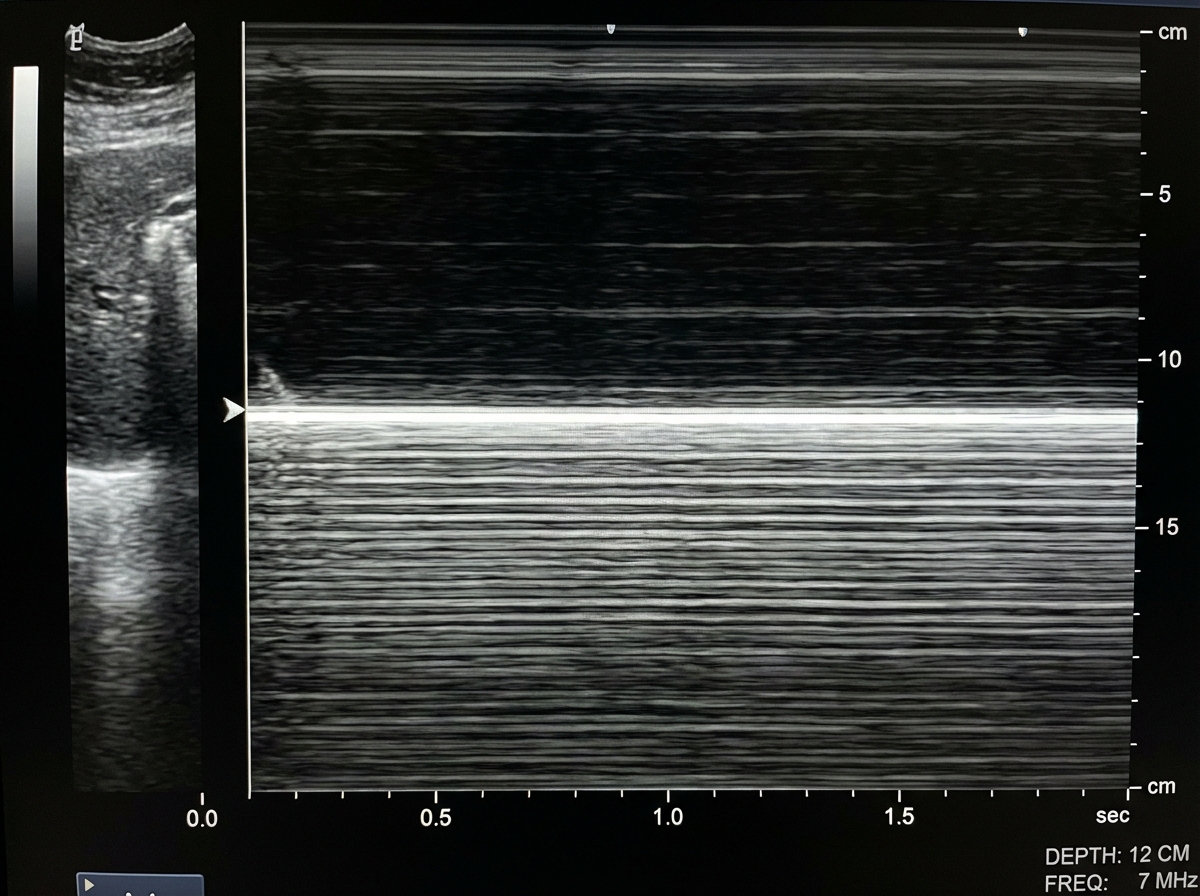
A patient presented with a history of blunt trauma to the chest and abdomen. On USG examination in M mode the following finding is seen. What is the likely diagnosis?
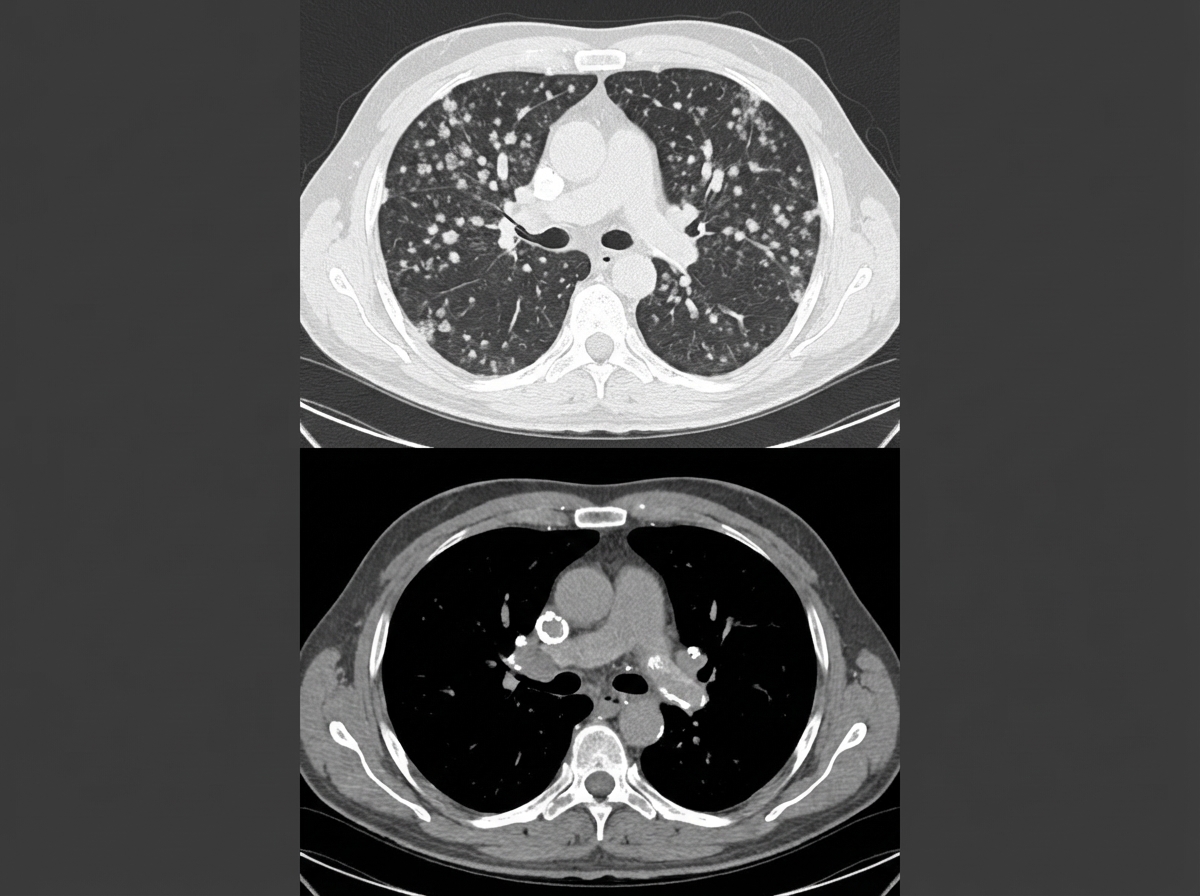
The following CT chest shows the presence of?
Atelectasis with reverse S sign is seen in which of the following conditions?
Perihilar fluffy opacities on chest X-ray are typically seen in which of the following conditions?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app