
Chest Radiology — MCQs

On this page
The "finger in glove" sign is seen in which of the following conditions?
What is the best investigation for diagnosing minimal right pleural effusion?
A chest X-ray shows Hilar vascular markings, Kerley B lines, and a hazy left lung field. What is the most likely diagnosis?
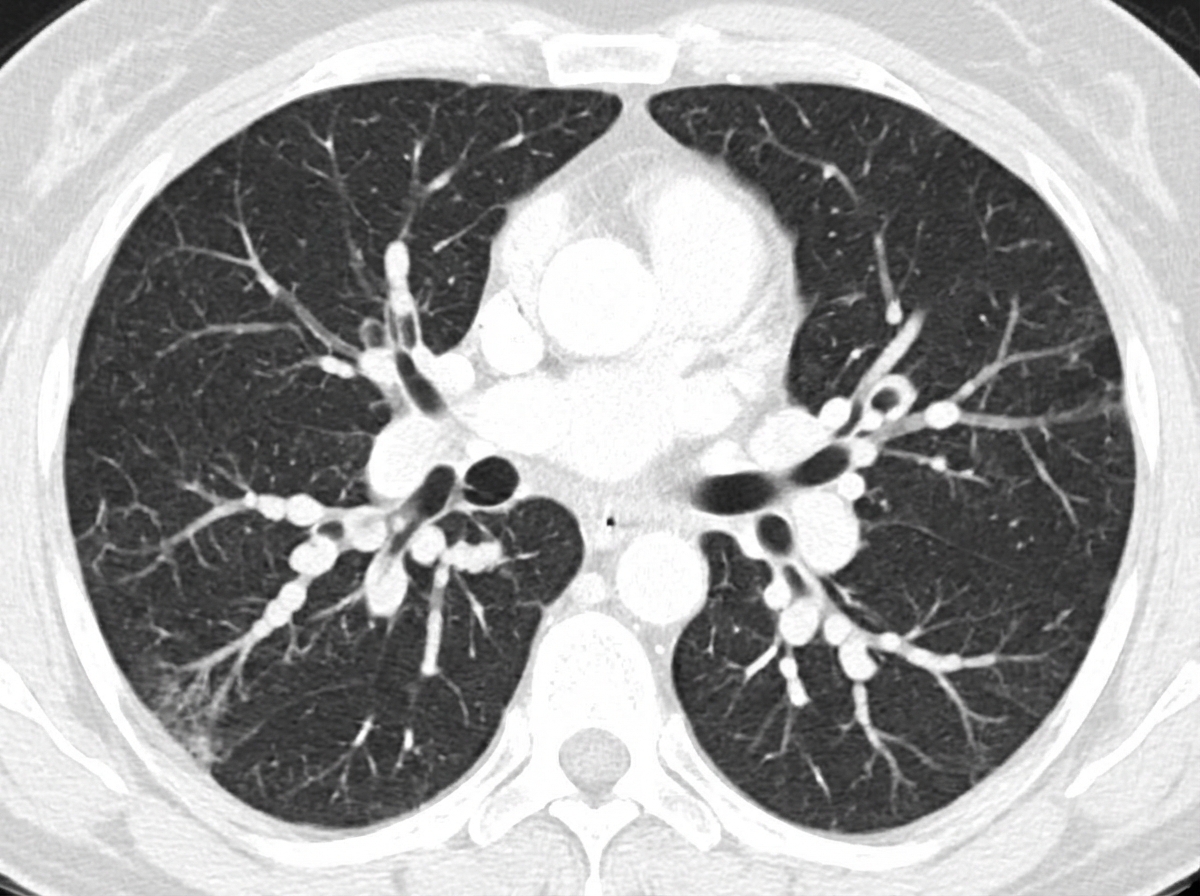
A patient presents with chronic productive cough and clubbing, with coarse rales on auscultation. What is the diagnosis suggested by the CT scan shown?
Kerley lines are typically seen in which of the following conditions?
Which of the following shows splaying of the carina in the retrocardiac shadow?
Which of the following statements about loculated pleural effusion is false?
What is the cause of posterior mediastinal opacity on a PA and lateral view of a chest X-ray?
Which of the following is NOT a true radiographic finding in emphysema?
Honey comb lung appearance is seen in which of the following conditions?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app