
Chest Radiology — MCQs

On this page
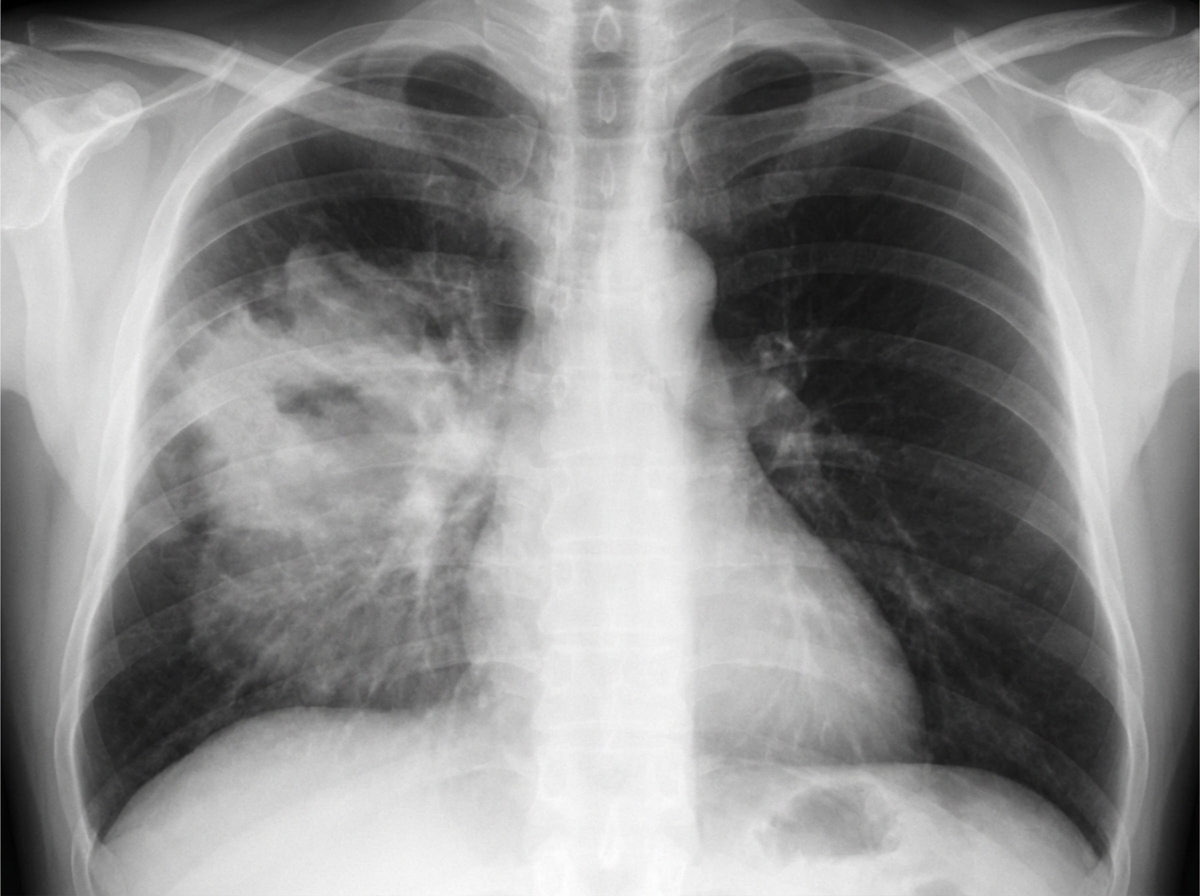
A 44-year-old man presents with dyspnea, cough, and mild pyrexia. Which lobe of the lung is most likely involved?
Which of the following is FALSE about Kerley's A lines?
The 'tree in bud' sign on HRCT is suggestive of which condition?
What is the best radiographic view for demonstrating an interlobar pleural effusion?
The "1-2-3 sign" or "Pawnbroker's sign" is typically seen in which of the following conditions?
Pulmonary mycetomas on radiographs most commonly show as?
The 'thumb print' sign is seen in which of the following conditions?
What imaging technique is best for demonstrating a small pneumothorax?
Which of the following features suggests a benign nature in the evaluation of a solitary pulmonary nodule on CT scan?
Sequestration lung is best diagnosed by?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app