
Chest Radiology — MCQs

On this page
Which of the following findings is NOT seen on HRCT in usual interstitial pneumonia (UIP)?
Which of the following conditions is associated with the presence of Kerley B lines on chest X-ray?
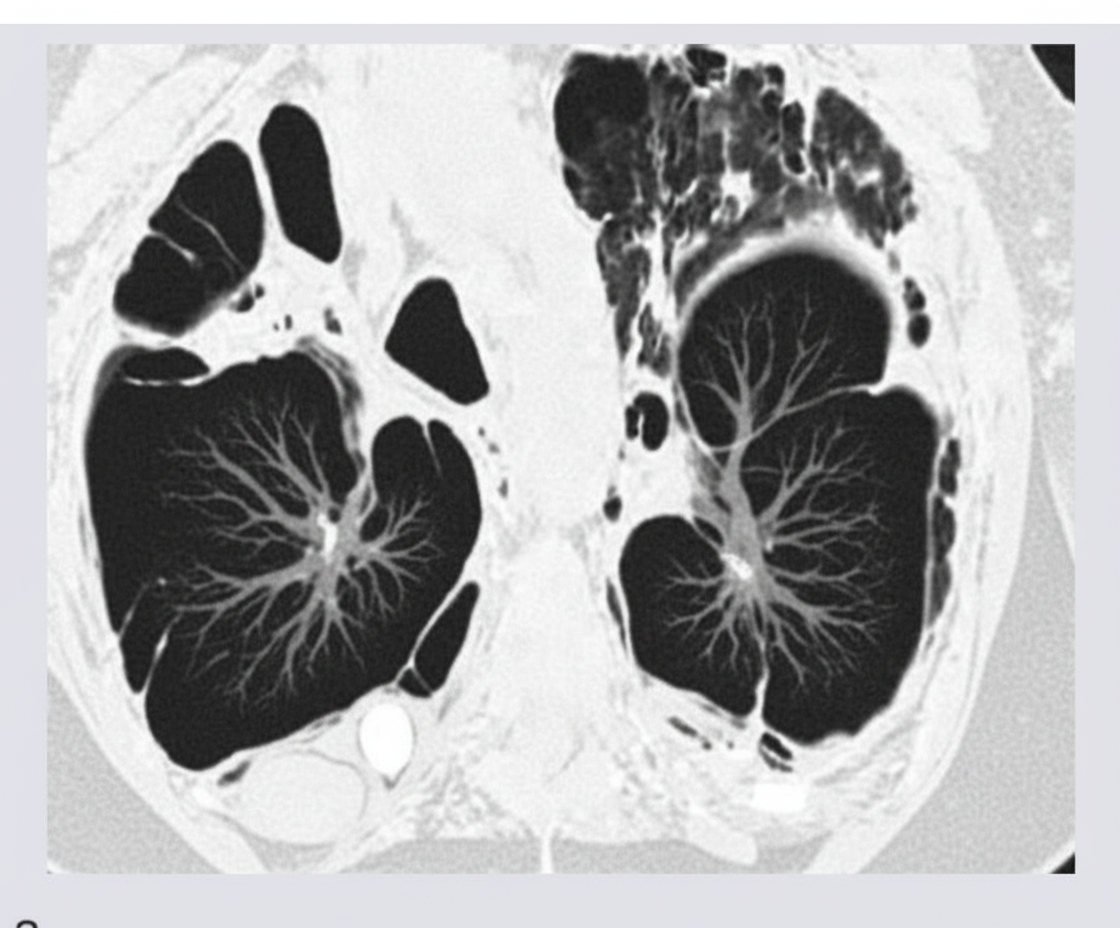
The following CT chest shows the presence of?
Water lilly appearance in a chest radiograph suggests which of the following conditions?
What condition is characterized by a 'dirty chest' appearance on a chest X-ray?
Evaluate the following statements regarding mediastinal masses and their evaluation: Thymoma is the most common anterior mediastinal mass. Neurogenic tumors are the most common posterior mediastinal masses. MRI is the investigation of choice to evaluate anterior and posterior mediastinal masses. Extramedullary hematopoiesis is a type of anterior mediastinal mass. A mediastinal mass forms an acute angle with the lung surface. Indicate whether each statement is True (T) or False (F).
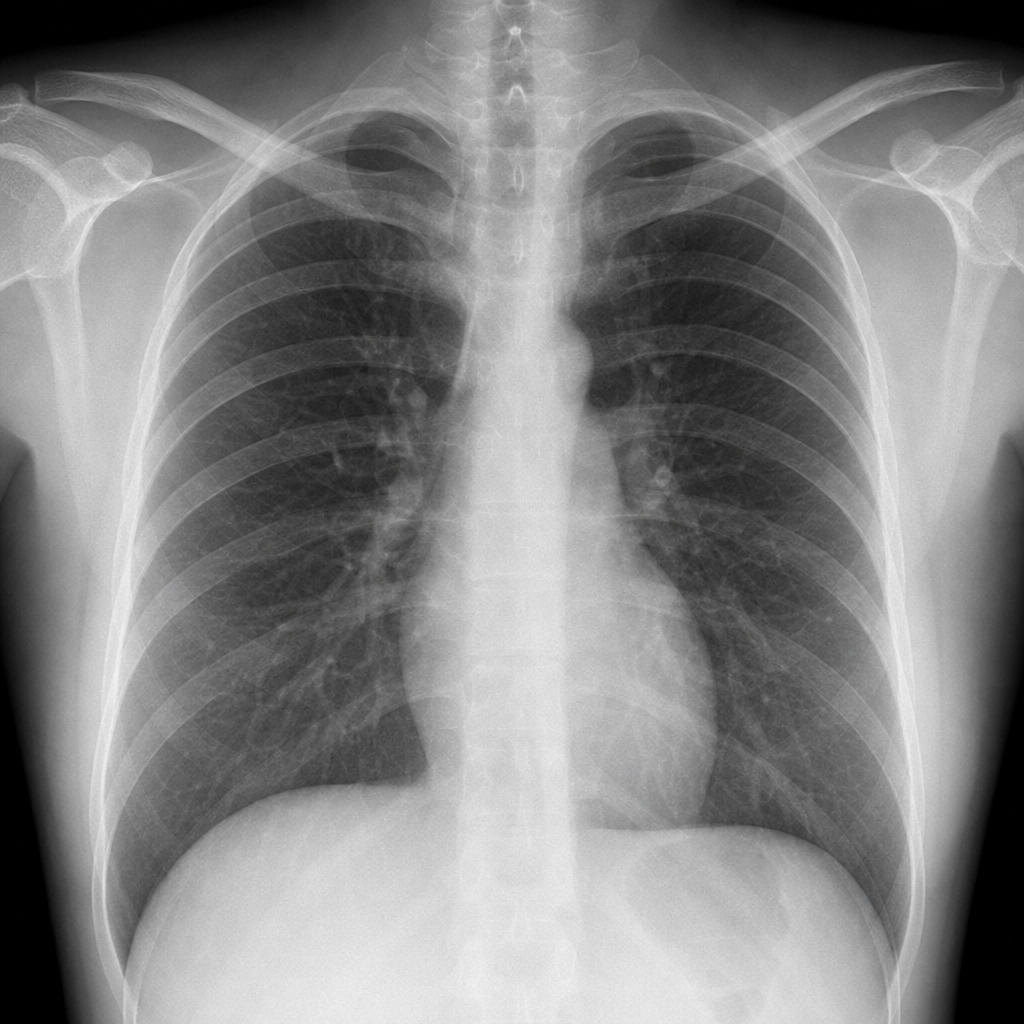
A 35-year-old female presents with chest pain and shortness of breath. The patient reports recent alcohol consumption with an episode of forceful retching and denies any history of trauma, similar episodes, smoking, or pulmonary tuberculosis. Her occupational history indicates unemployment for the past 6 months, previously working in an IT firm. On examination, there is focal tenderness over the right first rib. A chest X-ray has been performed. Which of the following statements is true regarding the management of the likely pathology?
The middle lobe of the lung is best visualized by which radiographic view?
Which X-ray view best demonstrates a right-sided pleural effusion?
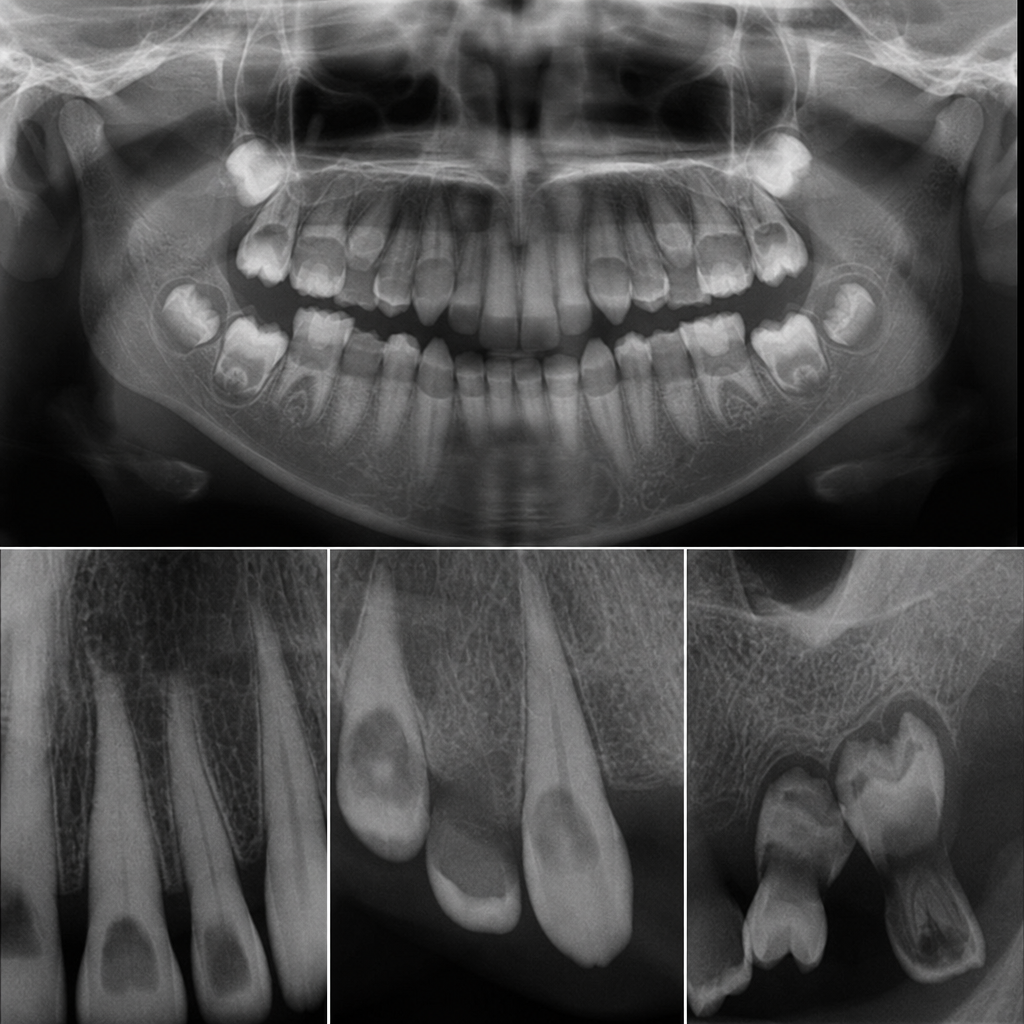
A radiograph shows an abnormal developmental condition of teeth. Which of the following is the most likely diagnosis based on typical radiographic findings?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app