
Chest Radiology — MCQs

On this page
A 12-year-old child presents with mild fever, runny nose, sore throat, and cough for 3 days. Clinical examination is consistent with an upper respiratory tract infection (URTI). There is no respiratory distress, oxygen desaturation, or focal chest findings. What is the most appropriate next step regarding imaging?
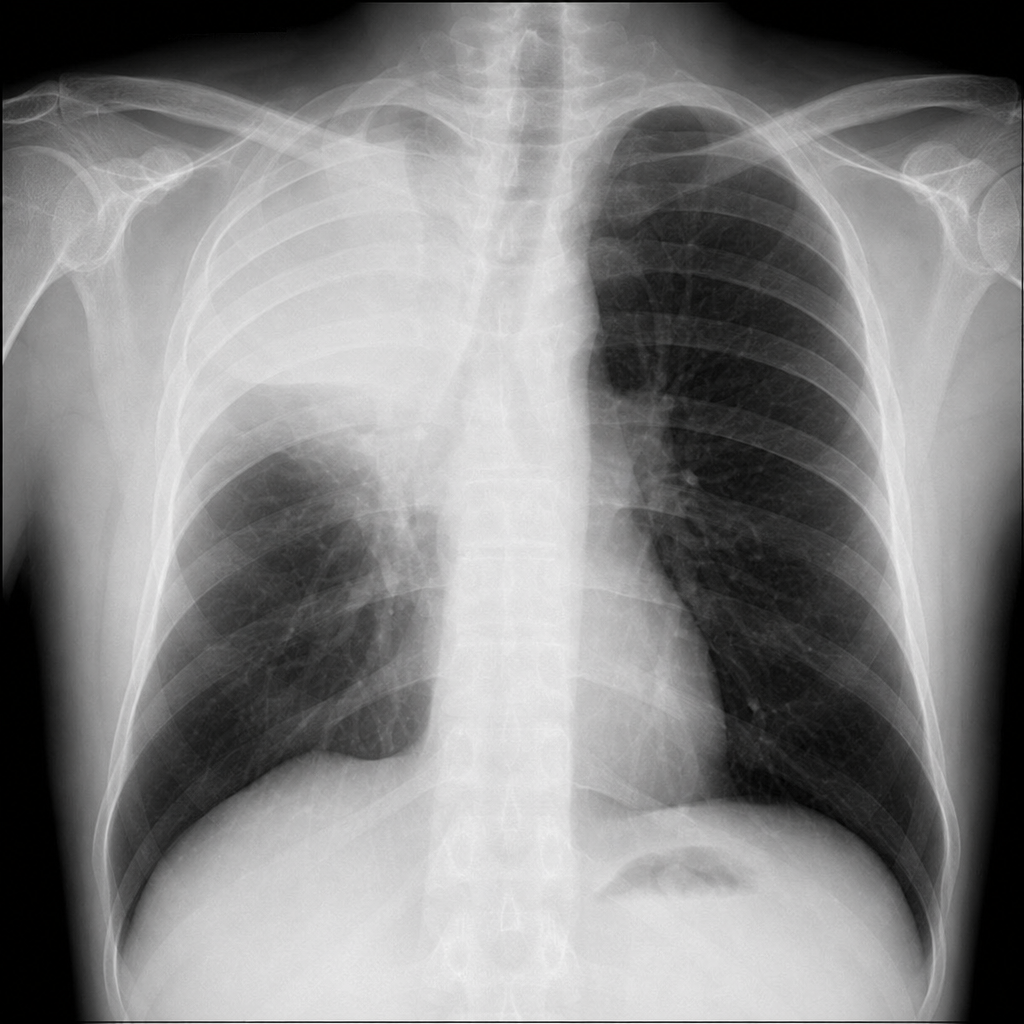
A 58-year-old male smoker presents with a 3-month history of progressive dyspnoea, haemoptysis, and 8 kg weight loss. Spirometry shows a mild obstructive pattern. Examination reveals reduced breath sounds at the right apex. A PA chest radiograph is shown in Image 2. Which of the following is the most likely diagnosis?
Mediastinal lymph node calcification is seen in which one of the following?
All of the following radiologic features are seen in patients with chronic cor pulmonale, except?
Non-visualization of the gastric fundic bubble in the retrocardiac region suggests which of the following?
Practice by Chapter
Normal Chest Radiographic Anatomy
Practice Questions
Radiographic Signs in Chest Imaging
Practice Questions
Pulmonary Infections
Practice Questions
Chronic Obstructive Pulmonary Disease
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Neoplasms
Practice Questions
Pleural Diseases
Practice Questions
Mediastinal Pathology
Practice Questions
Congenital and Developmental Chest Anomalies
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Chest Trauma Imaging
Practice Questions
Post-Surgical Chest Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app