
Cardiovascular Radiology — MCQs

On this page
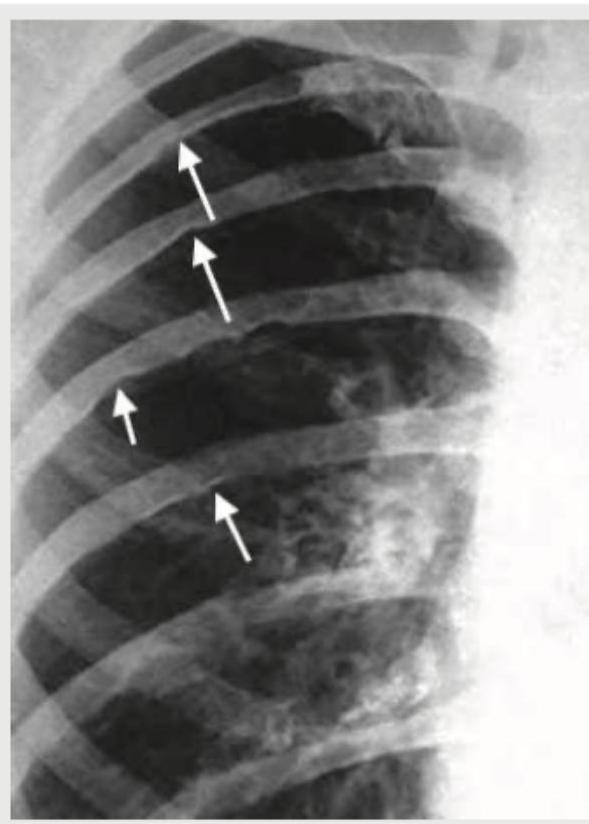
In the condition shown below, rib notching is present in which of the following ribs? (AIIMS Nov 2015)
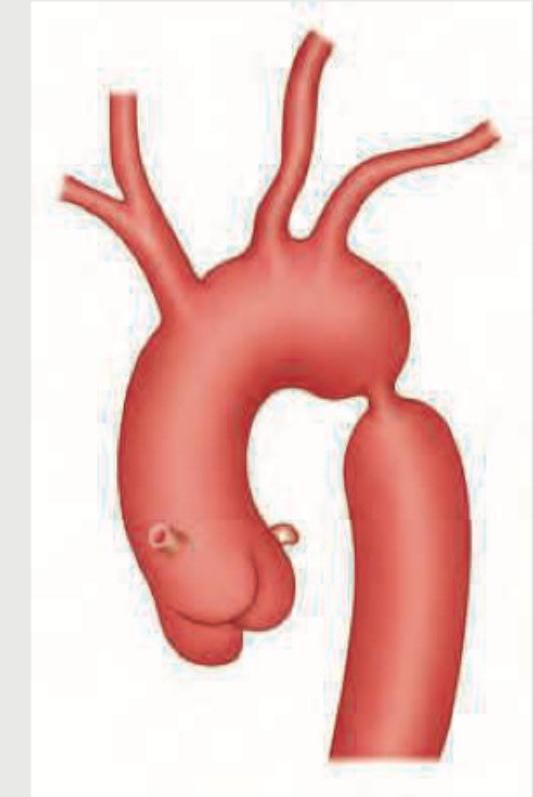
A short stature female presents with history of wearing socks in summer season. Physical examination shows icy cold toes with diminished femoral pulses and lower-extremity hypotension compared to the upper extremities. CXR done shows:
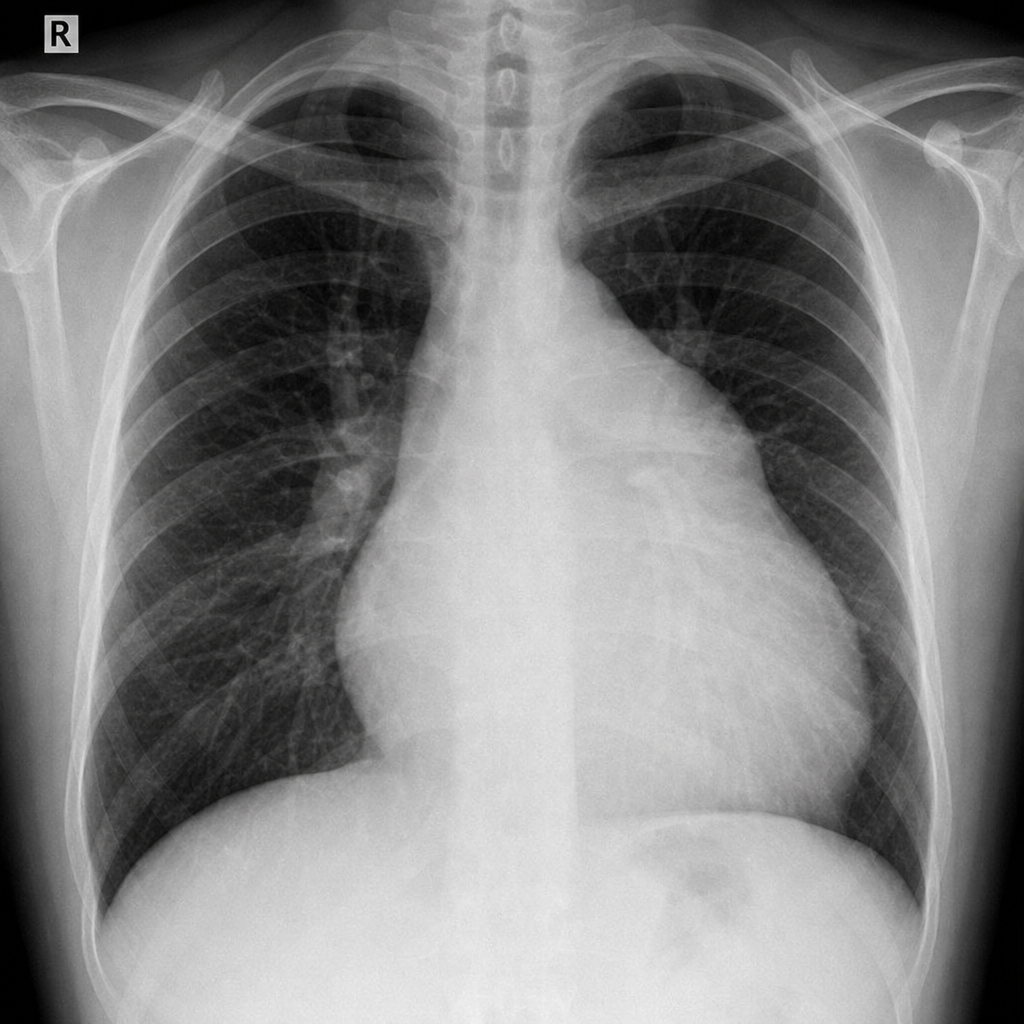
A 35-year-old hypertension patient has the following CXR in annual medical check up. What does it show?

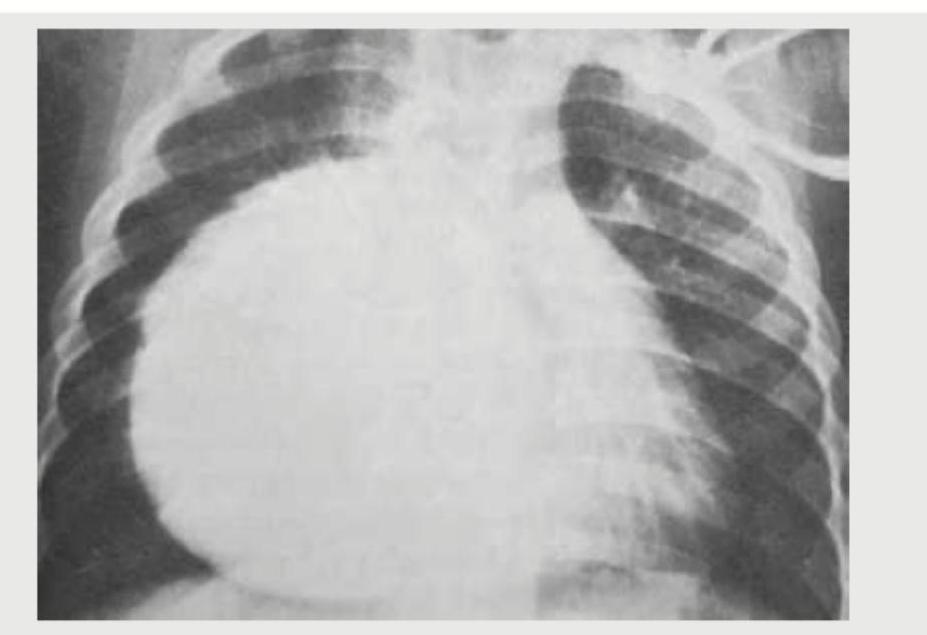
Identify the congenital heart disease presenting with cyanosis in CXR: (Recent NEET Pattern 2016-17)
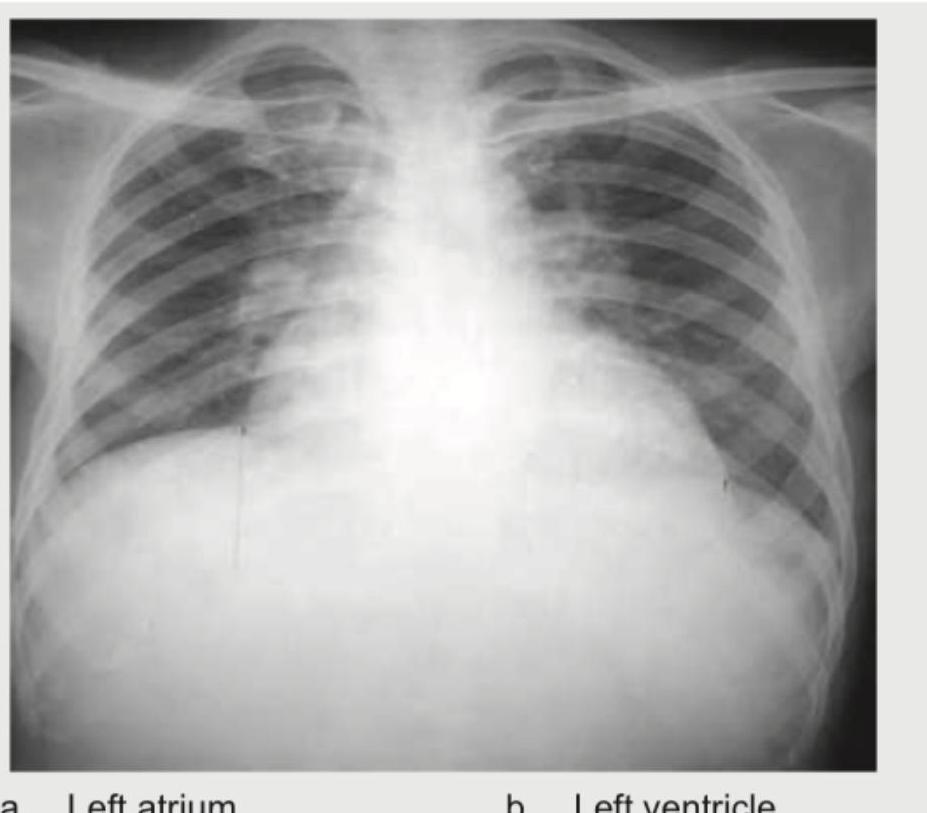
In the chest X-ray shown, identify the chamber enlargement:

A chest X-ray (PA view) shows cardiomegaly. Identify the chamber enlargement:
In the chest X-ray shown below, identify the chamber enlargement:
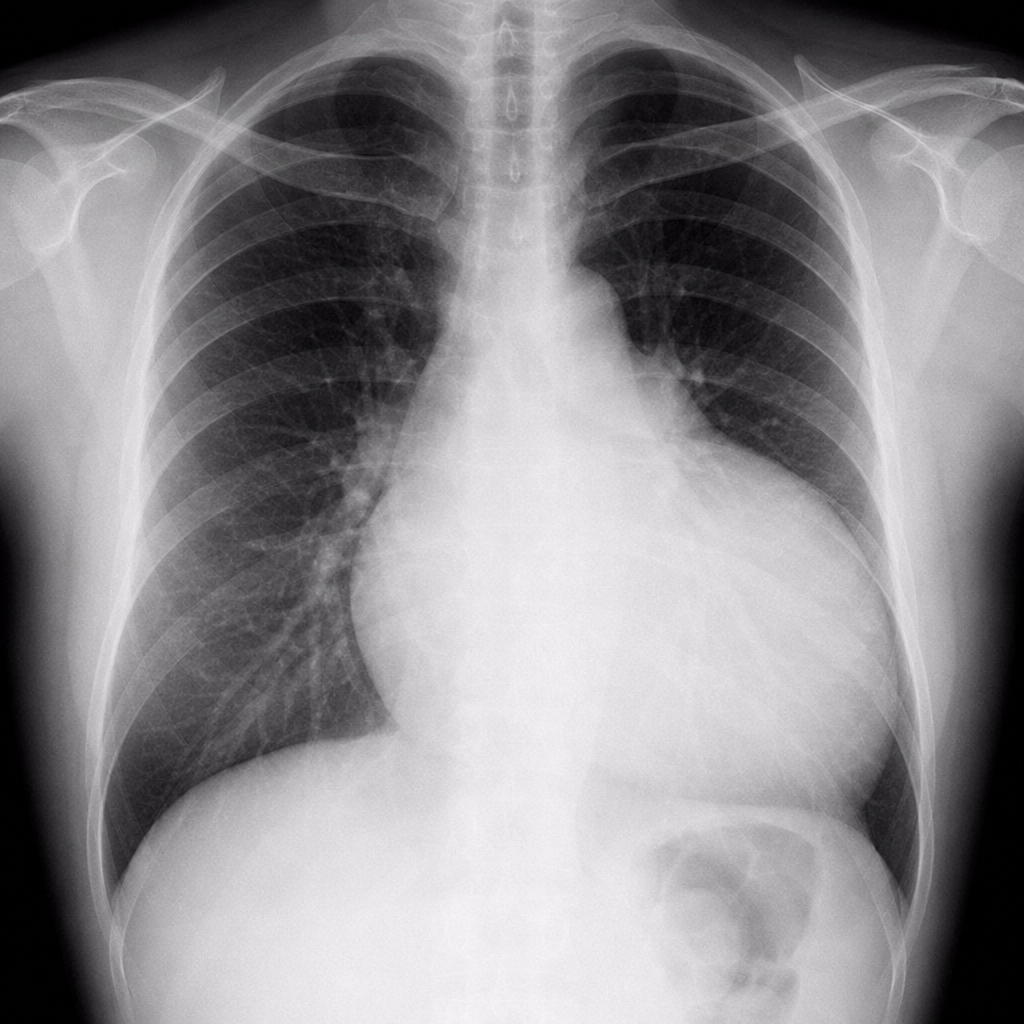
A 30-year-old hypertension patient presents with daily headaches. The CXR given below shows which of the following? (Recent NEET Pattern 2016-17)

Identify the chamber enlargement:
A chest X-ray shows the following appearance. What is the most likely diagnosis based on the radiographic appearance?

Practice by Chapter
Cardiovascular Anatomy
Practice Questions
Cardiac CT Techniques
Practice Questions
Cardiac MRI Techniques
Practice Questions
Ischemic Heart Disease Imaging
Practice Questions
Valvular Heart Disease
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease
Practice Questions
Aortic and Great Vessel Imaging
Practice Questions
Peripheral Vascular Imaging
Practice Questions
Cardiovascular Interventional Procedures
Practice Questions
Post-Surgical Cardiovascular Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app