
Cardiovascular Radiology — MCQs

On this page
Globular heart with plethoric lung fields is seen in which condition?
In which aspect is transesophageal echocardiography superior to transthoracic echocardiography?
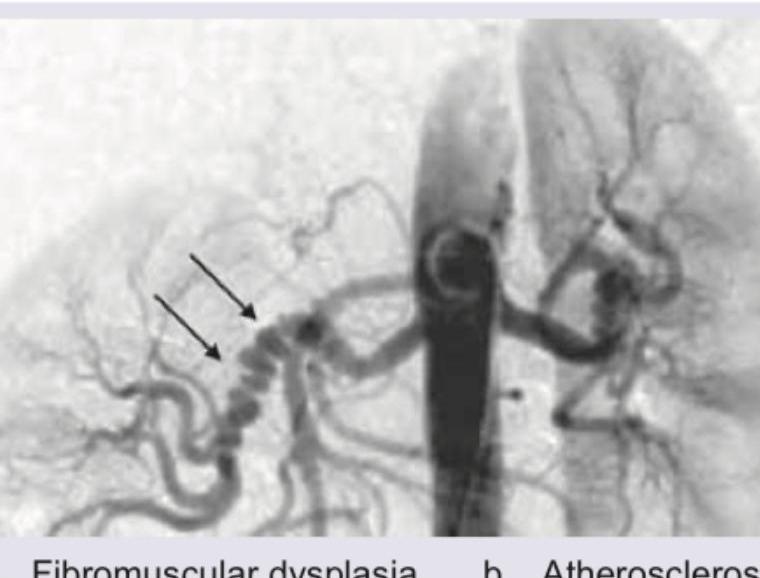
Which condition is most likely associated with the following angiography findings?

What is the most important sign of significance of renal artery stenosis on an angiogram?
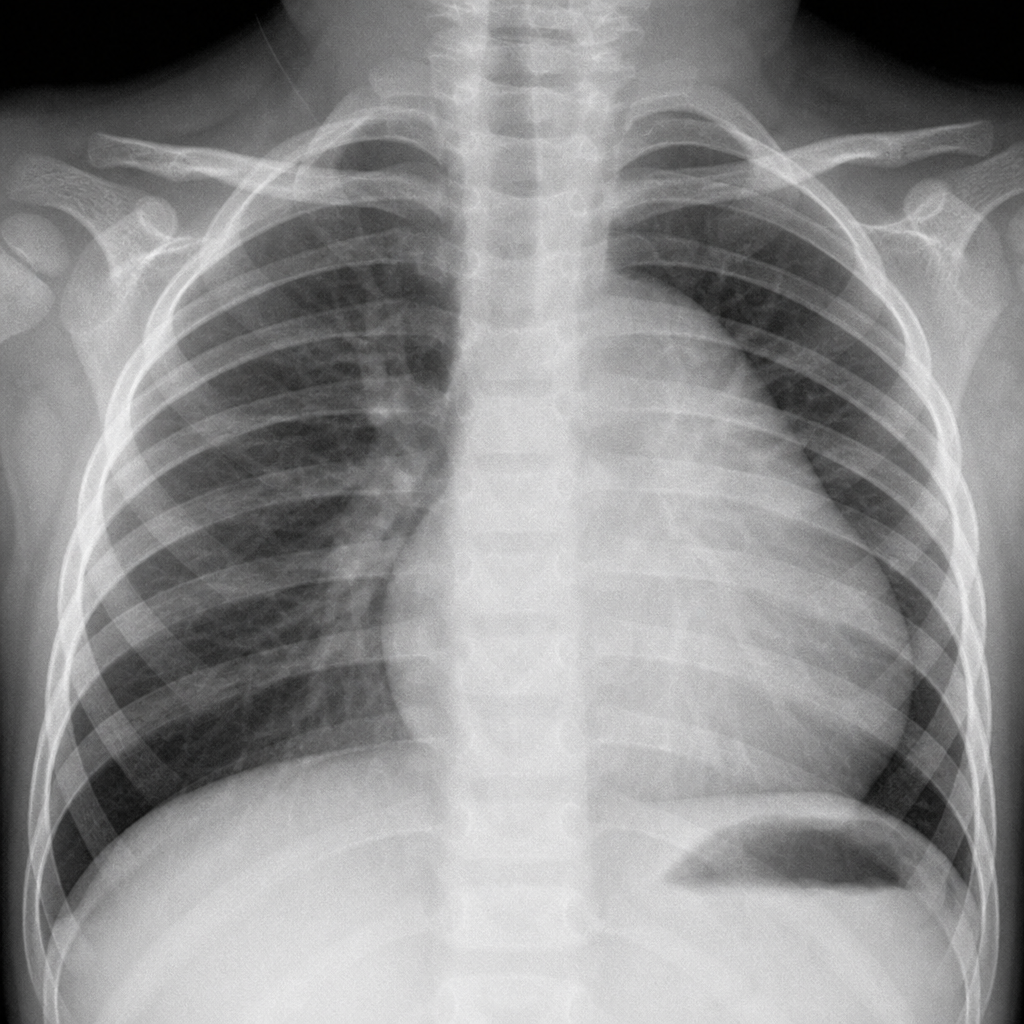
A newborn presents with cyanosis, a pansystolic murmur loudest at the lower left sternal border, and echocardiography showing apical displacement of the tricuspid valve leaflets with severe tricuspid regurgitation and massive right atrial enlargement. This x-ray is suggestive of what condition?
The 'egg on its side' appearance of the heart on a radiograph is characteristic of which congenital heart anomaly?
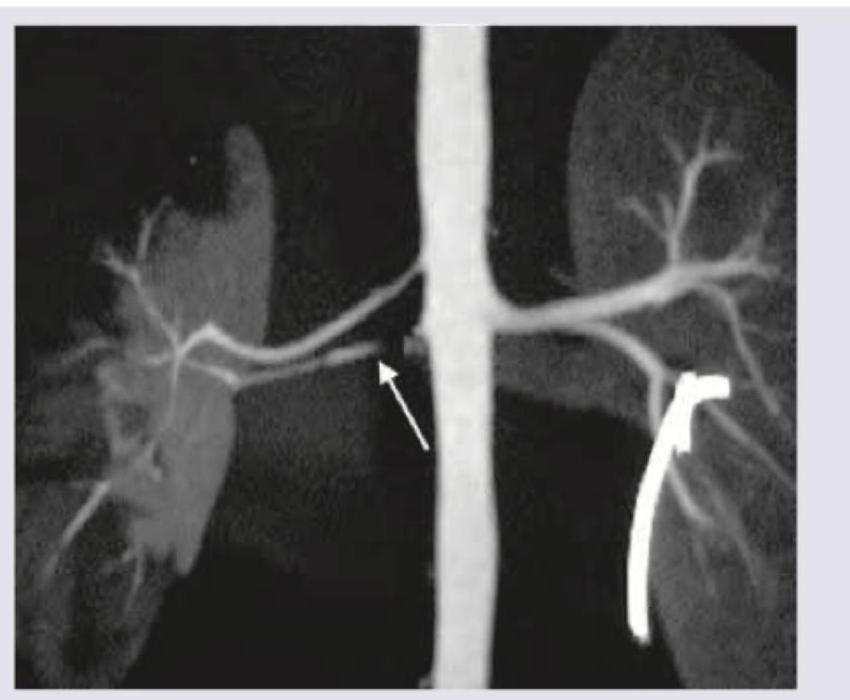
What is the most likely underlying cause of the arterial abnormality shown in the CT angiography image?
One-month-old child with tet spells. Incorrect about the image shown?

What does the following angiogram in a hypertension patient show?
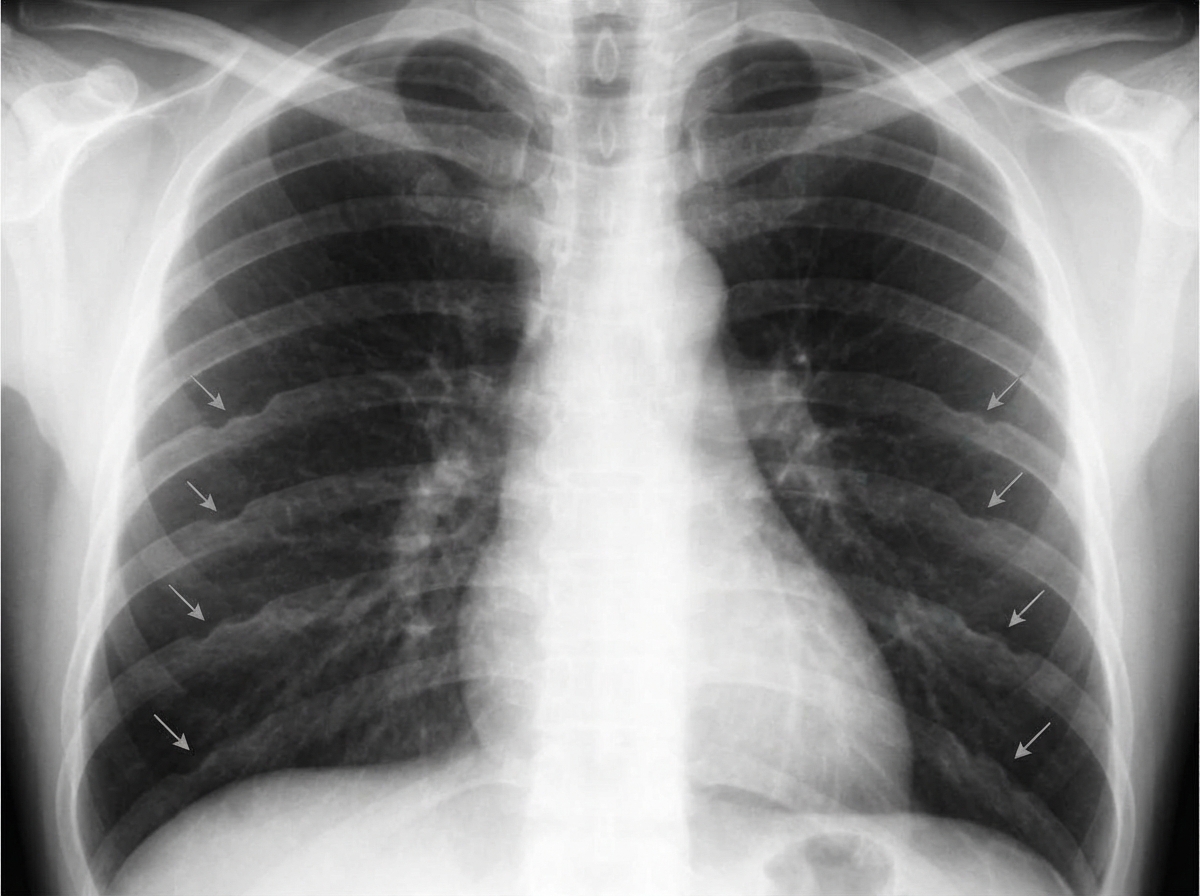
What condition is suggested by inferior rib notching in a setting of hypertension?
Practice by Chapter
Cardiovascular Anatomy
Practice Questions
Cardiac CT Techniques
Practice Questions
Cardiac MRI Techniques
Practice Questions
Ischemic Heart Disease Imaging
Practice Questions
Valvular Heart Disease
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease
Practice Questions
Aortic and Great Vessel Imaging
Practice Questions
Peripheral Vascular Imaging
Practice Questions
Cardiovascular Interventional Procedures
Practice Questions
Post-Surgical Cardiovascular Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app