
Cardiovascular Radiology — MCQs

On this page
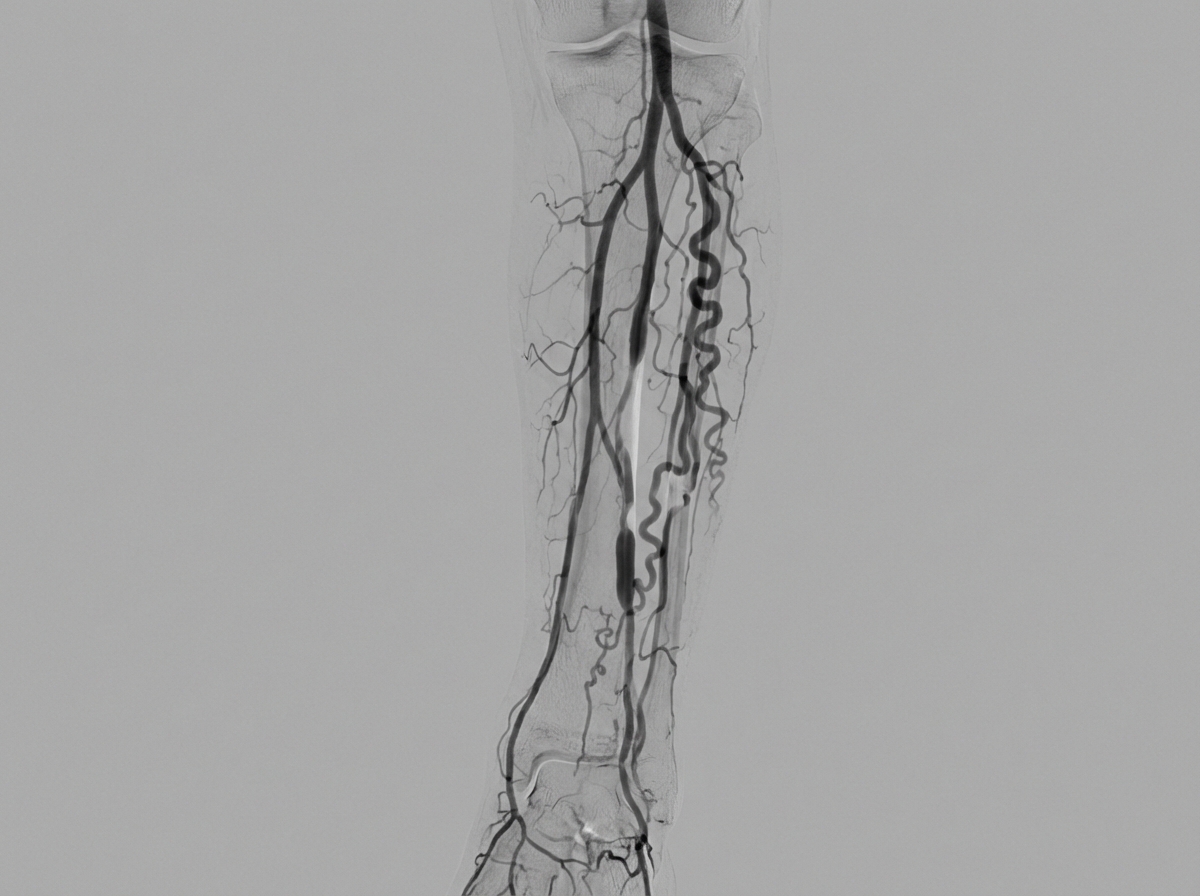
A digital subtraction angiography of a 35-year-old smoker is shown. What is the possible diagnosis?
Cardiac CT is best performed during which phase of the cardiac cycle?
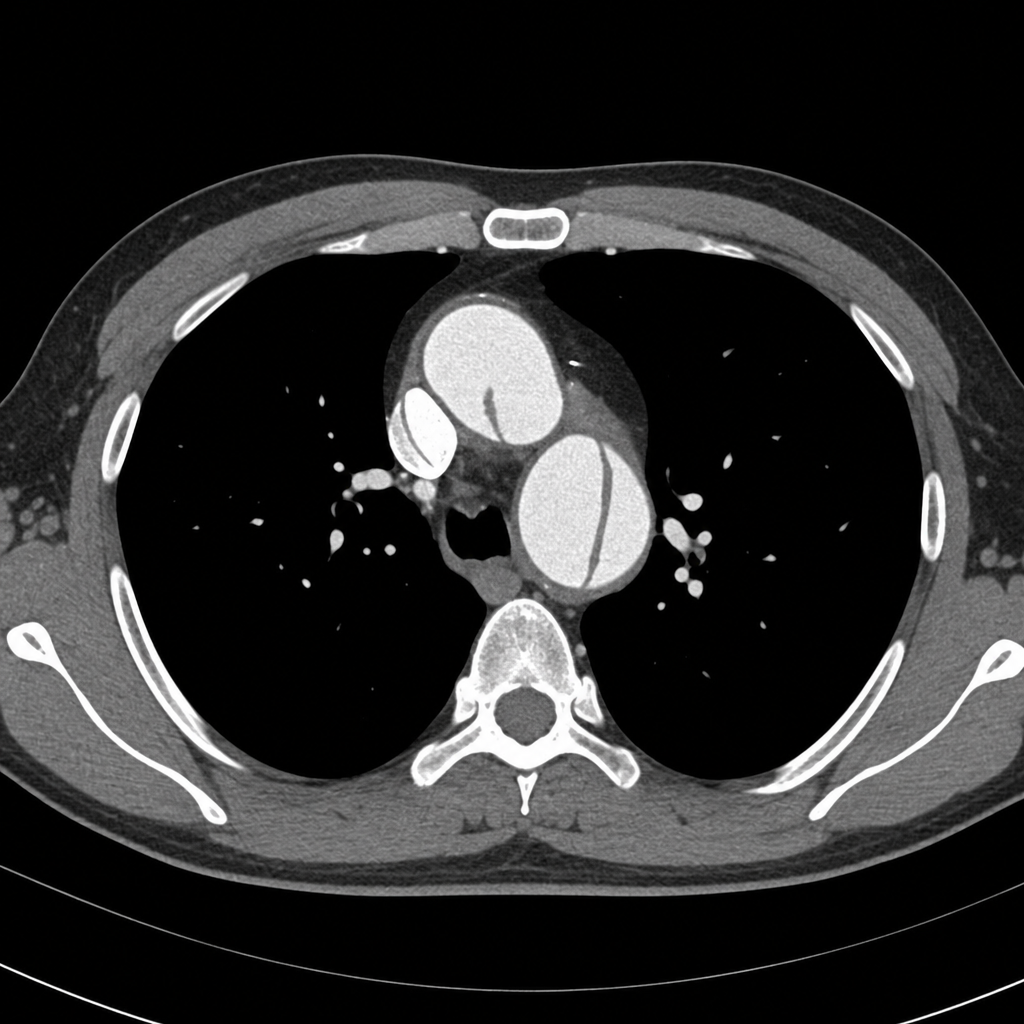
Which description best identifies the abnormality shown on this axial CT angiogram?
Which imaging modality is used to diagnose a vascular ring causing external airway compression?
Which condition is characterized by an "egg in cup" appearance on imaging?
The "Inveed Moustache Sign" is seen in which of the following conditions?
Which technique is not recently used to check for disorder or patency of coronary artery circulation?
Which imaging modality is best for assessing plaque morphology in atherosclerosis?
Ground glass appearance of the ventricular septum is seen in which of the following conditions?
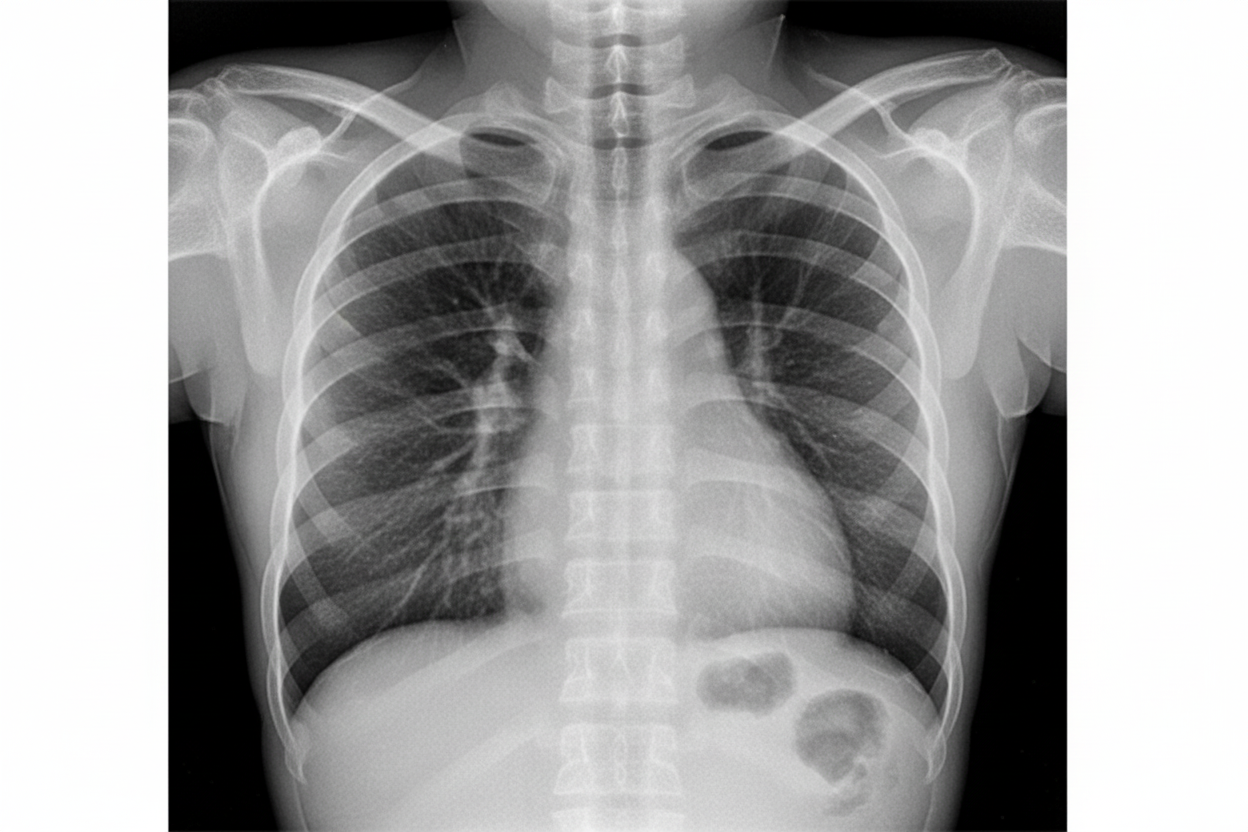
What is the likely diagnosis based on the provided chest X-ray?
Practice by Chapter
Cardiovascular Anatomy
Practice Questions
Cardiac CT Techniques
Practice Questions
Cardiac MRI Techniques
Practice Questions
Ischemic Heart Disease Imaging
Practice Questions
Valvular Heart Disease
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease
Practice Questions
Aortic and Great Vessel Imaging
Practice Questions
Peripheral Vascular Imaging
Practice Questions
Cardiovascular Interventional Procedures
Practice Questions
Post-Surgical Cardiovascular Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app