
Cardiovascular Radiology — MCQs

On this page
Which is the best investigation for assessing the plaque of atherosclerosis?
A 63-year-old patient with a history of tachyarrhythmias is on an implantable cardioverter-defibrillator (ICD). The patient suddenly develops shock. Which of the following is the best investigation to assess the position and integrity of the ICD?
In which of the following conditions is an increased cardiac silhouette NOT seen, except?
A "water can" appearance of the heart shadow in a Chest X-ray is seen in which of the following conditions?
What is the characteristic radiographic appearance of aoitis?
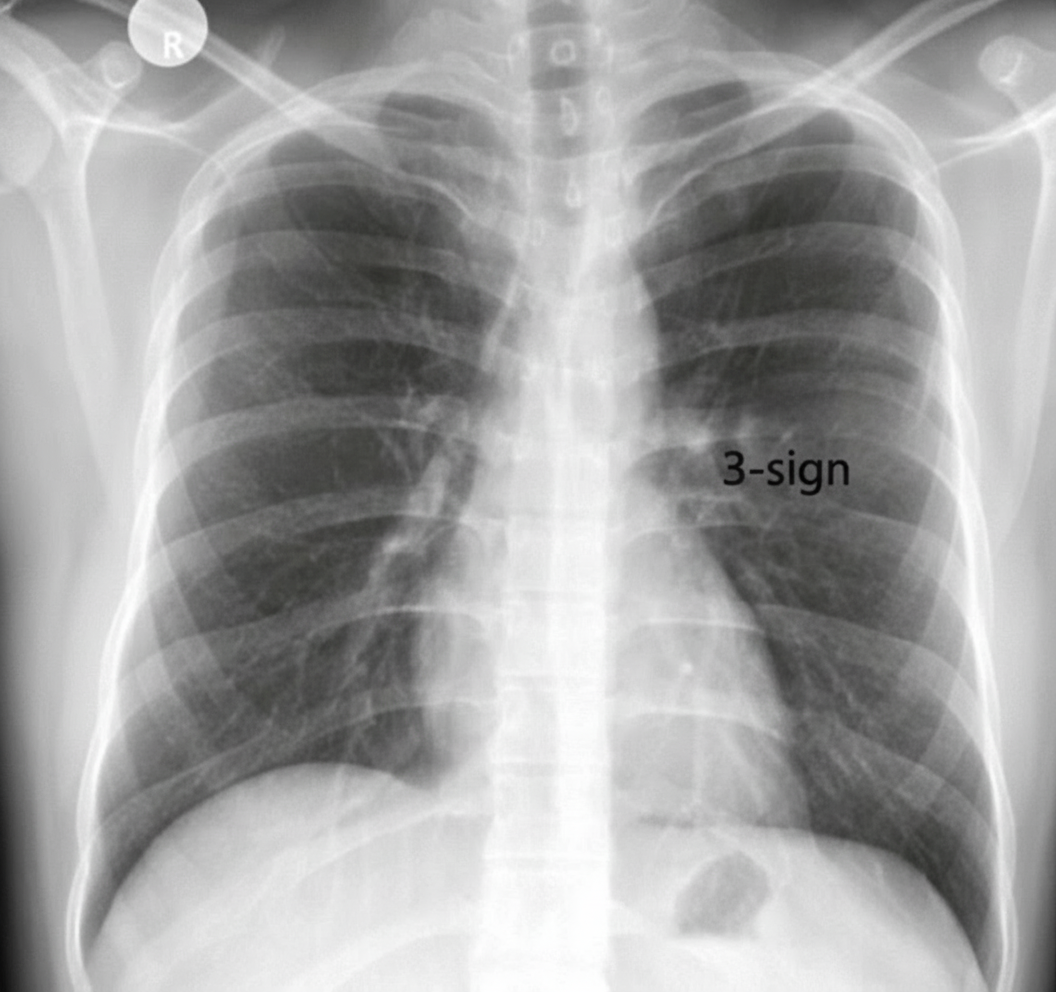
Which of the following statements is FALSE regarding Coarctation of the Aorta?
A chest radiograph is obtained from a male patient with hypertension. What is the probable diagnosis?
What is the investigation of choice to confirm hemochromatosis as the cause of cardiomyopathy?
Which of the following is the most common feature of aortitis on chest x-ray?
In which of the following conditions is a 'Coeur-en-Sabot' (boot-shaped) heart seen?
Practice by Chapter
Cardiovascular Anatomy
Practice Questions
Cardiac CT Techniques
Practice Questions
Cardiac MRI Techniques
Practice Questions
Ischemic Heart Disease Imaging
Practice Questions
Valvular Heart Disease
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease
Practice Questions
Aortic and Great Vessel Imaging
Practice Questions
Peripheral Vascular Imaging
Practice Questions
Cardiovascular Interventional Procedures
Practice Questions
Post-Surgical Cardiovascular Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app