
Cardiovascular Radiology — MCQs

On this page
All of the following are features of chest radiography in Tetralogy of Fallot except?
What is the diagnostic method for dysphagia lusoria?
Egg on side appearance in chest x-ray is seen in which of the following conditions?
Hilar dance on fluoroscopy is seen in which condition?
In mitral stenosis, a double atrial shadow is due to enlargement of which chamber?
Which of the following is NOT seen in left atrial enlargement?
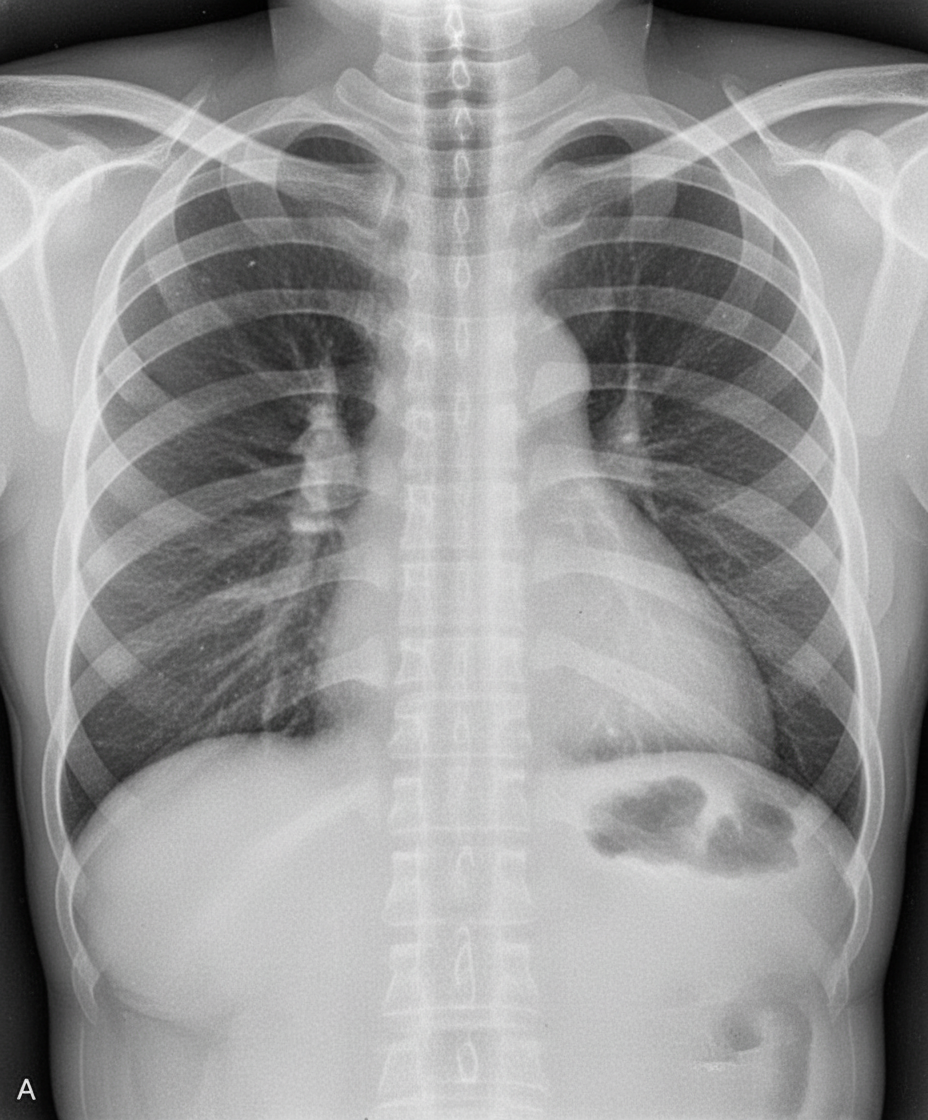
The given x-ray is suggestive of which of the following conditions?
Which of the following radiological signs is NOT typically seen in a patient with mitral stenosis?
An X-ray of an asymptomatic 64-year-old male executive, who had an anterior Q wave myocardial infarction 4 years ago, shows a persistent bulge in the left ventricular contour. What is your diagnosis?
In atrial septal defect, what is the typical state of the aorta?
Practice by Chapter
Cardiovascular Anatomy
Practice Questions
Cardiac CT Techniques
Practice Questions
Cardiac MRI Techniques
Practice Questions
Ischemic Heart Disease Imaging
Practice Questions
Valvular Heart Disease
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease
Practice Questions
Aortic and Great Vessel Imaging
Practice Questions
Peripheral Vascular Imaging
Practice Questions
Cardiovascular Interventional Procedures
Practice Questions
Post-Surgical Cardiovascular Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app