
Cardiovascular Radiology — MCQs

On this page
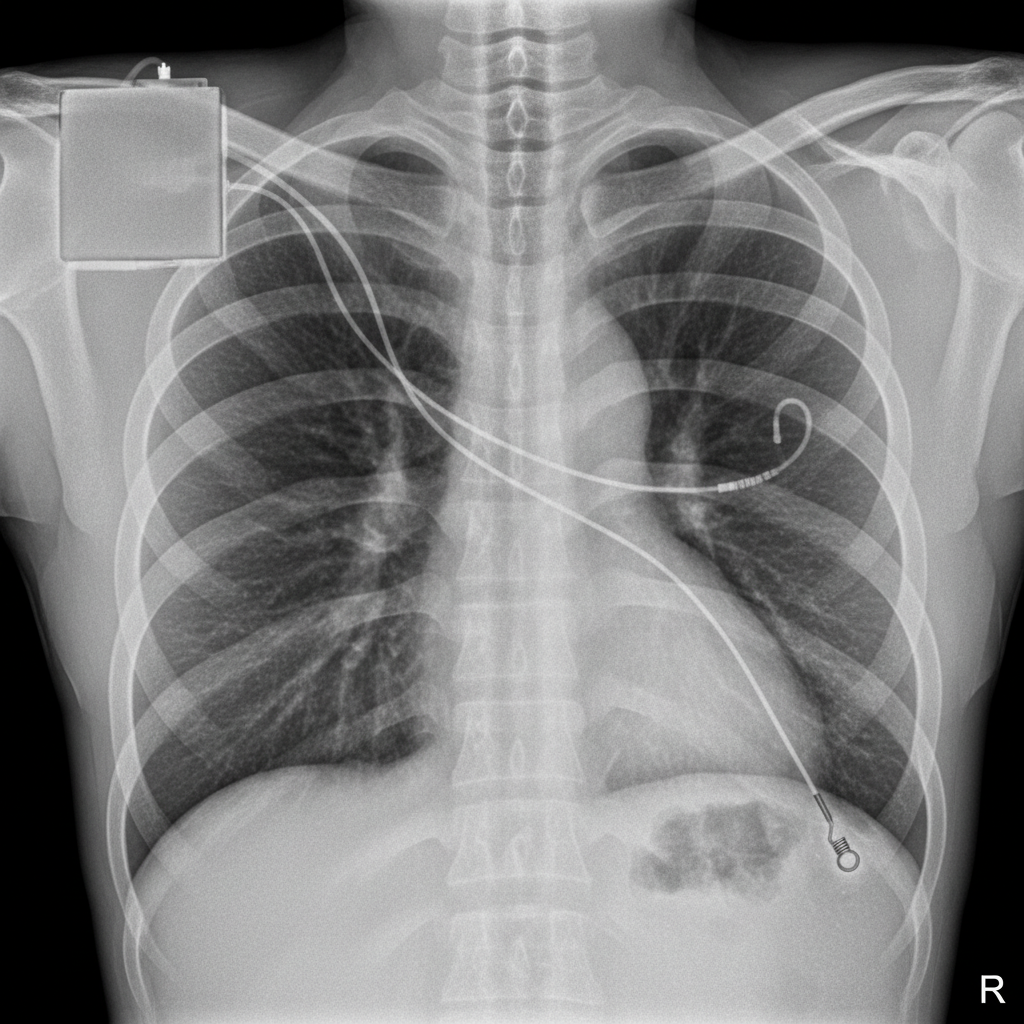
What is the location of the atrial and ventricular pacemaker lead tips, respectively?
What is the typical movement of mitral valve calcification?
What is the radiological finding of a "sitting duck heart"?
What is the procedure of choice for the evaluation of aortic aneurysm?
A 68-year-old woman presented with unstable angina and underwent cardiac catheterization by radial access. There was difficulty advancing the guidewire; a brachial angiogram revealed the following. What is the diagnosis?

'Spade-like' deformity of the cardiac apex on angiography is pathognomonic of:
String of beads appearance on angiography is seen in which of the following conditions?
The investigation of choice in aortic dissection is:
Comment on the diagnosis of the patient?

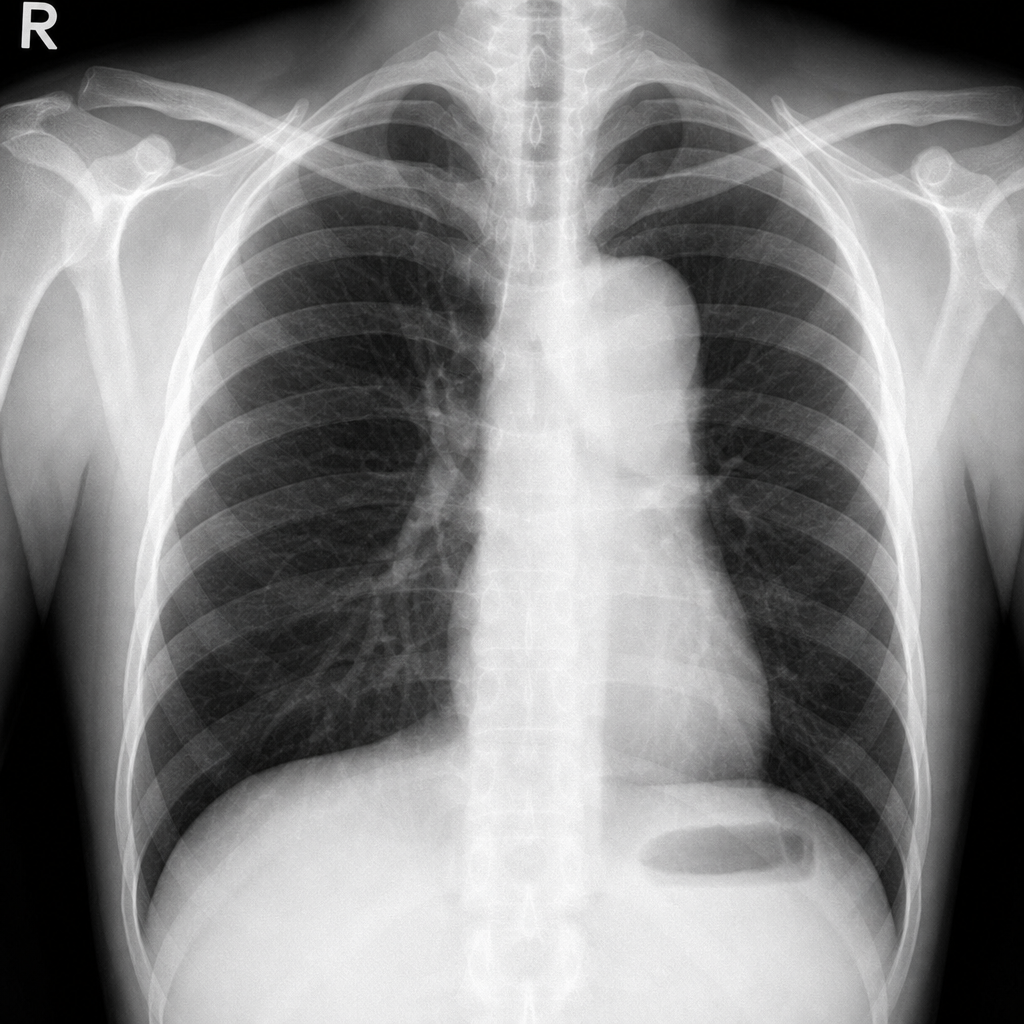
A 20-year-old man with hypertension presents with the following chest X-ray finding showing a figure-3 aortic contour. What could be the cause of this aortic shadow?
Practice by Chapter
Cardiovascular Anatomy
Practice Questions
Cardiac CT Techniques
Practice Questions
Cardiac MRI Techniques
Practice Questions
Ischemic Heart Disease Imaging
Practice Questions
Valvular Heart Disease
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease
Practice Questions
Aortic and Great Vessel Imaging
Practice Questions
Peripheral Vascular Imaging
Practice Questions
Cardiovascular Interventional Procedures
Practice Questions
Post-Surgical Cardiovascular Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app