
Cardiovascular Radiology — MCQs

On this page
Left atrial enlargement is best seen with which imaging view?
Which condition is characterized by the presence of the figure of three signs?
A left-sided cardiac bulge seen on chest X-ray is most likely due to which of the following?
Transesophageal echocardiogram (TEE) is superior to transthoracic echocardiogram (TTE) because of which of the following advantages?
What is the procedure of choice for the evaluation of an aortic aneurysm?
Which of the following statements is TRUE about Coronary Calcium Scoring, EXCEPT?
Which of the following is NOT a radiological sign of coarctation of the aorta?
Which is the most accurate investigation for assessing left ventricular global systolic function?
Hilar dance is seen in fluoroscopy of which condition?
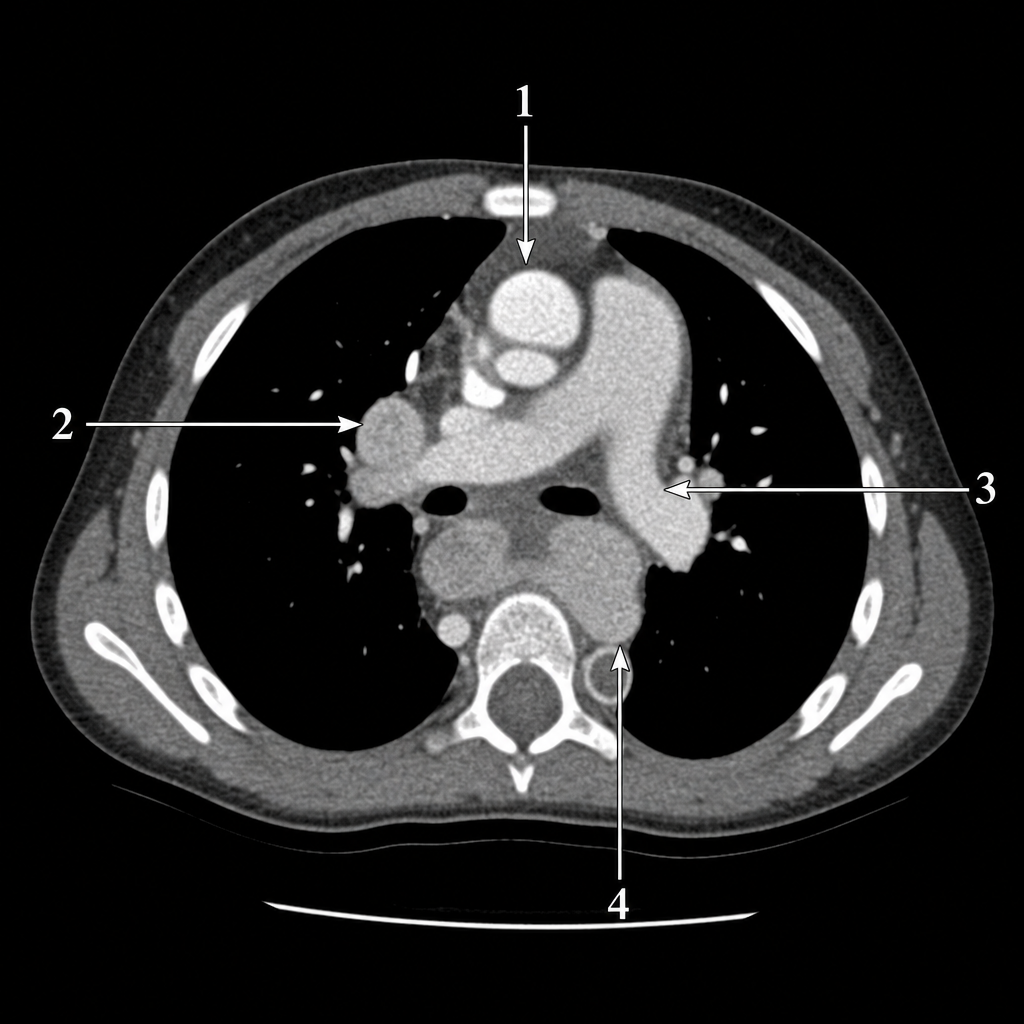
A preterm neonate presents for follow-up with a systolic murmur, tachypnea, and hepatomegaly. Further history reveals the mother had an episode of fever with rash during the antenatal period. If CECT were performed, which of the following marked areas would represent a probable pathology in this neonate?
Practice by Chapter
Cardiovascular Anatomy
Practice Questions
Cardiac CT Techniques
Practice Questions
Cardiac MRI Techniques
Practice Questions
Ischemic Heart Disease Imaging
Practice Questions
Valvular Heart Disease
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease
Practice Questions
Aortic and Great Vessel Imaging
Practice Questions
Peripheral Vascular Imaging
Practice Questions
Cardiovascular Interventional Procedures
Practice Questions
Post-Surgical Cardiovascular Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app