
Cardiovascular Radiology — MCQs

On this page
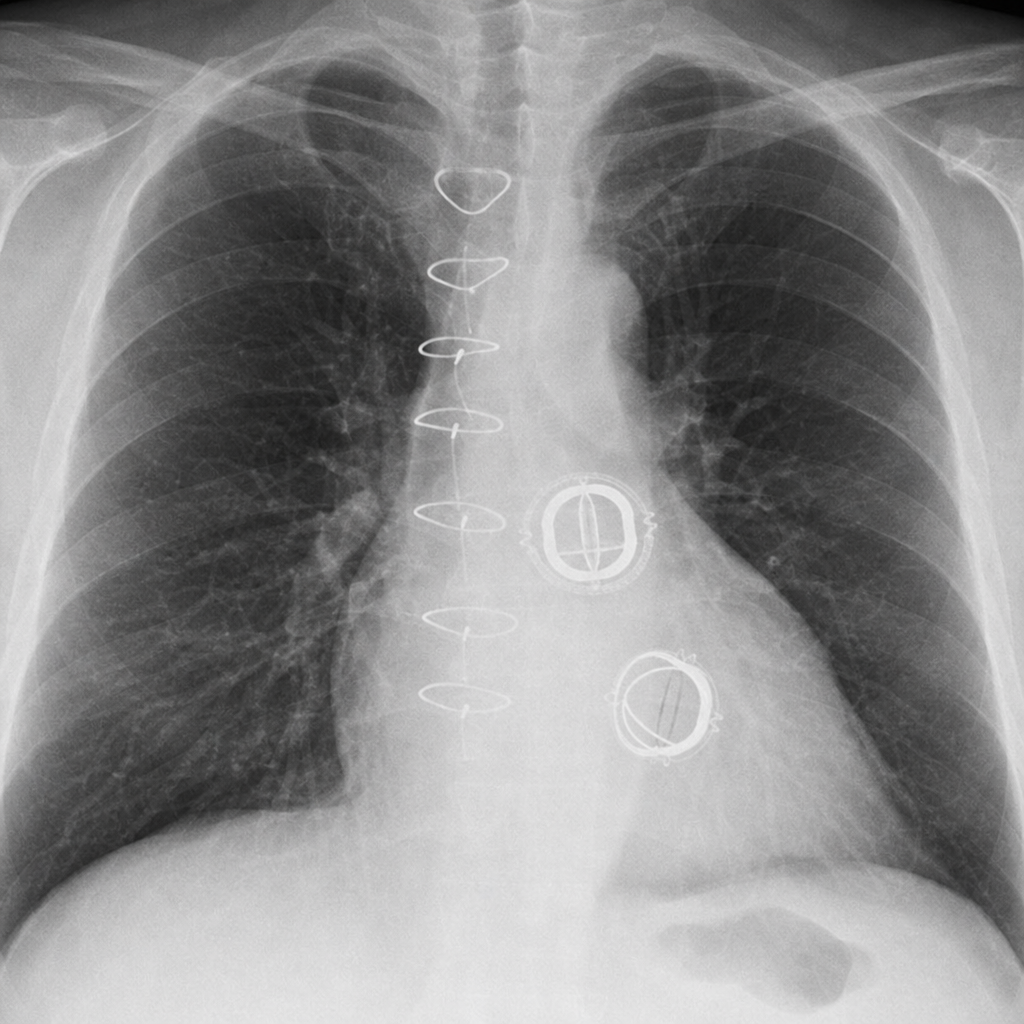
Which cardiac valves have been replaced?
Inferior rib notching is seen in all of the following conditions except:
An 8-year-old child has exertional cyanosis, reduced exercise tolerance, and episodic palpitations. Examination reveals a holosystolic murmur at the left lower sternal border that becomes louder with inspiration. ECG shows right bundle-branch block with ventricular pre-excitation. The chest radiograph shown demonstrates moderate cardiomegaly without pulmonary edema. Which congenital heart defect is most likely?

The 'Oreo cookie sign' is a radiological finding suggestive of which of the following conditions?
What is the best investigation for diagnosing an abdominal aortic aneurysm?
The plain X-ray chest finding that suggests syphilitic cardiovascular disease is:
Inferior rib notching is characteristically present in which of the following congenital cardiac anomalies?
X-ray features of Atrial Septal Defect (ASD) are all except:
A patient with mitral stenosis will show all of the following findings on chest imaging except?
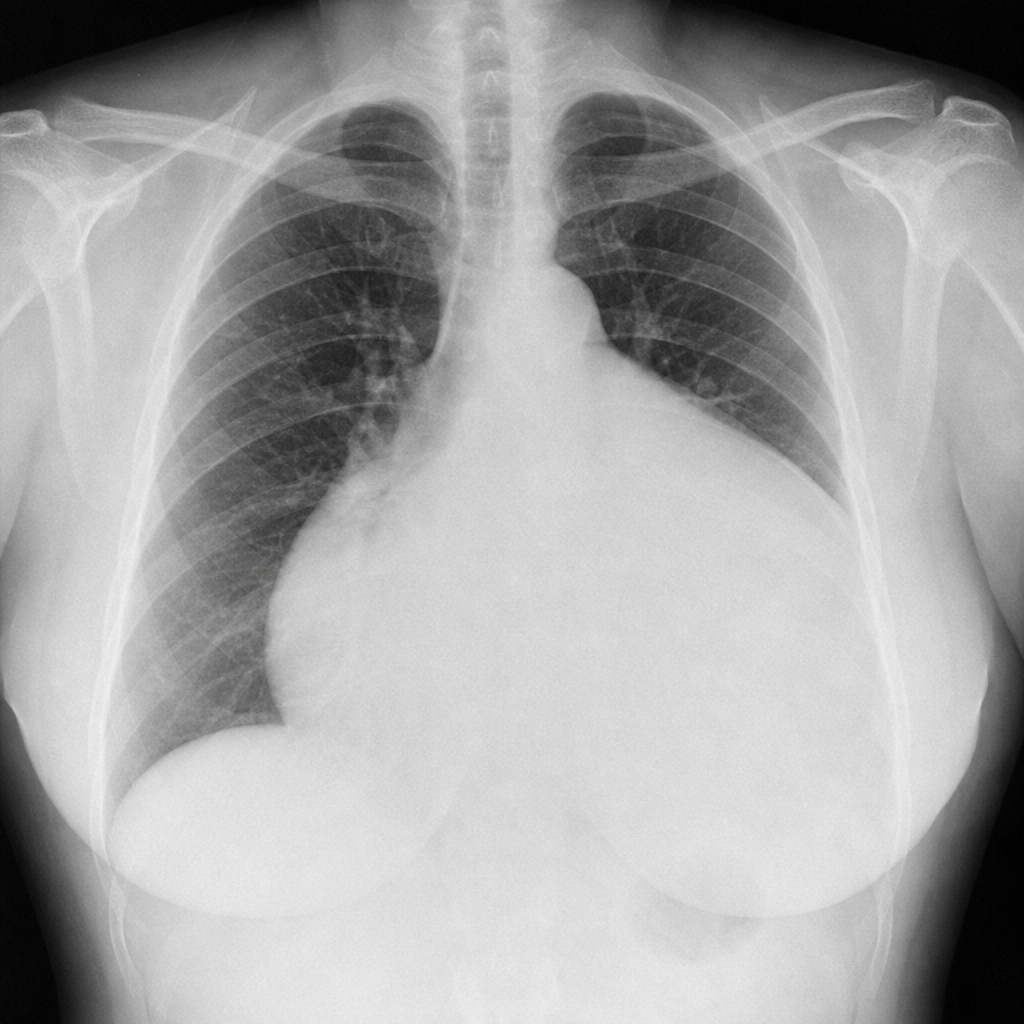
A 48-year-old female presented with dyspnea, chest pain, and a feeling of pressure on her chest. A CXR was ordered as part of her investigations. The patient had a normal CXR 5 months ago with normal heart size. Which of the following is the most probable diagnosis?
Practice by Chapter
Cardiovascular Anatomy
Practice Questions
Cardiac CT Techniques
Practice Questions
Cardiac MRI Techniques
Practice Questions
Ischemic Heart Disease Imaging
Practice Questions
Valvular Heart Disease
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease
Practice Questions
Aortic and Great Vessel Imaging
Practice Questions
Peripheral Vascular Imaging
Practice Questions
Cardiovascular Interventional Procedures
Practice Questions
Post-Surgical Cardiovascular Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app