
Cardiovascular Radiology — MCQs

On this page
Flask shaped heart is seen in –
The procedure of choice for the evaluation of an aneurysm is:
Gas shadow in the heart and great vessels is characteristically seen in:
Snowman sign is seen in:
Egg on side appearance is seen in:
Carotid atheromas may appear radiographically as:
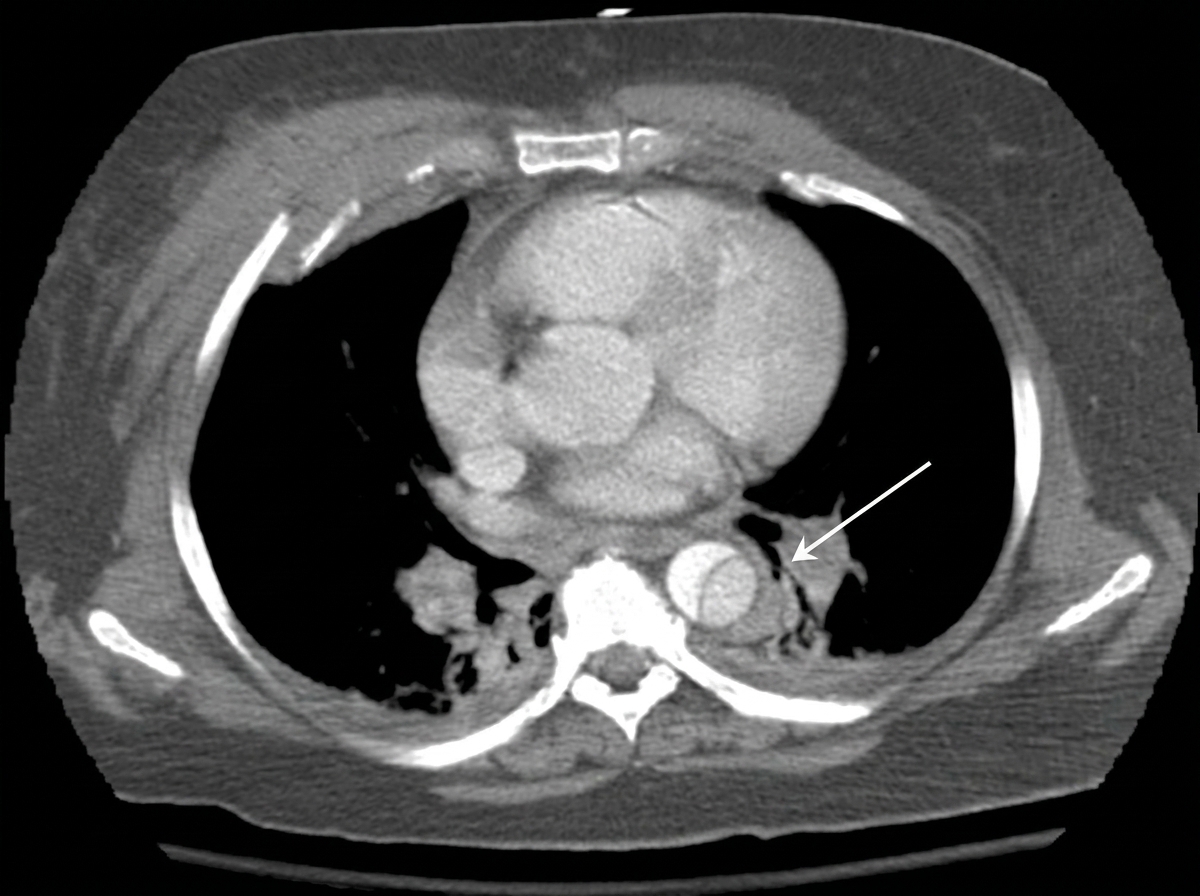
The CT thorax image shows:
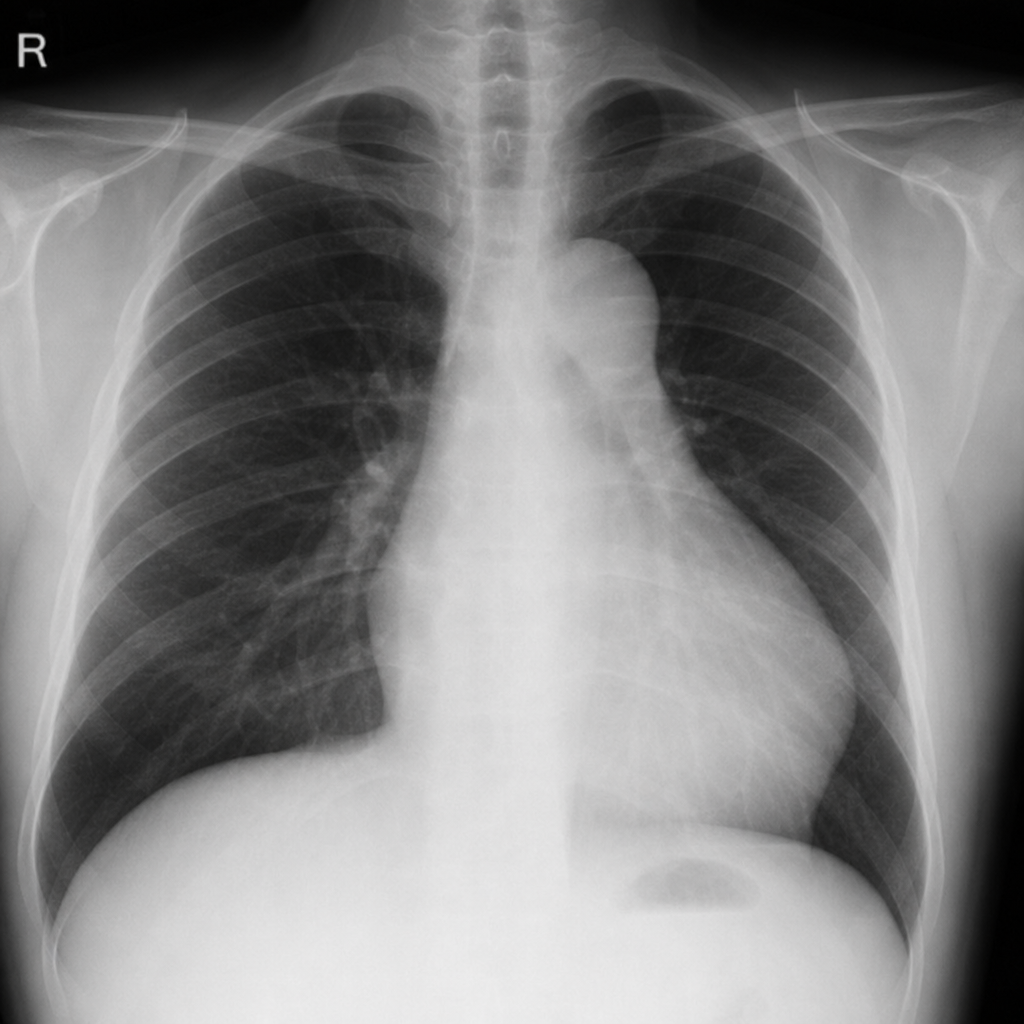
The Figure of 3 sign on chest X-ray is seen in which condition?
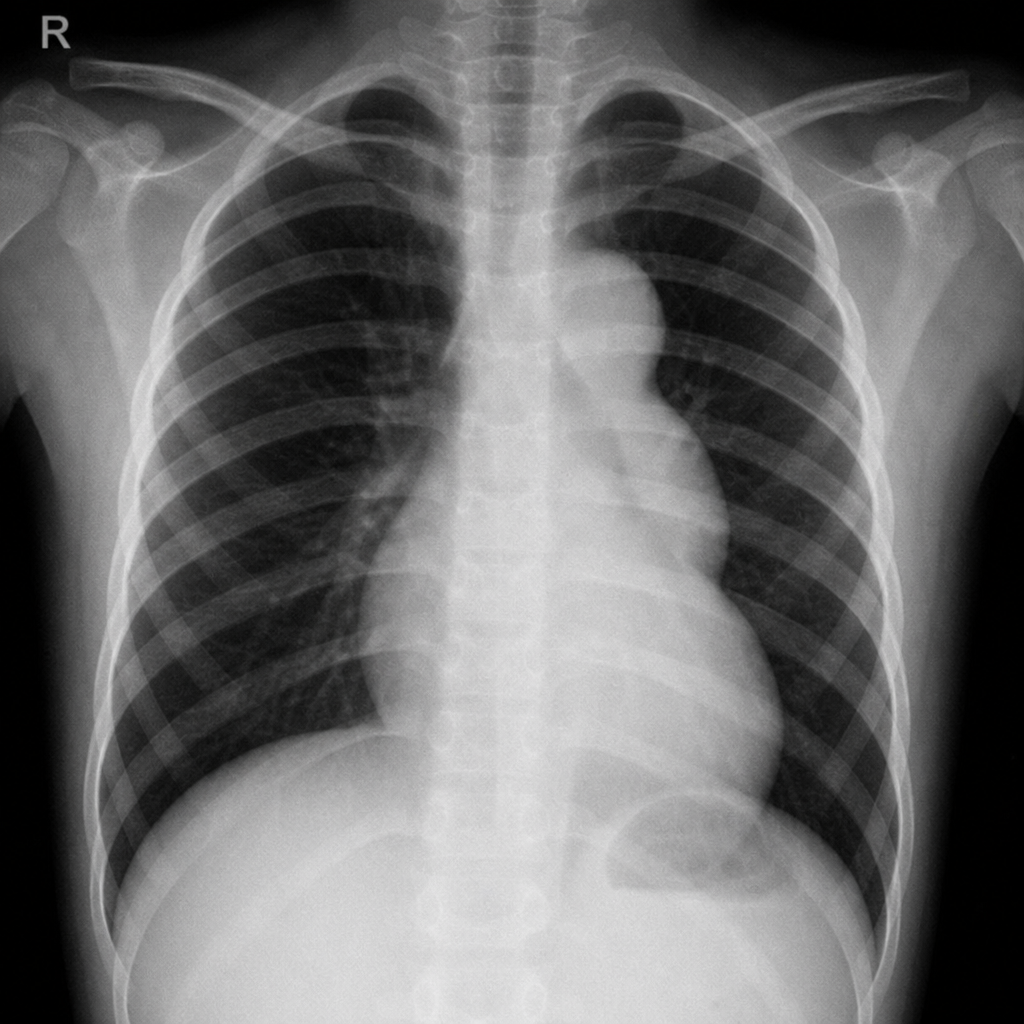
A male patient presents with hypertension, upper-extremity blood pressure significantly higher than lower-extremity blood pressure, and delayed femoral pulses. What could be the probable diagnosis?
Which of the following is the most reliable imaging technique for detecting cyanotic congenital heart diseases in newborns?
Practice by Chapter
Cardiovascular Anatomy
Practice Questions
Cardiac CT Techniques
Practice Questions
Cardiac MRI Techniques
Practice Questions
Ischemic Heart Disease Imaging
Practice Questions
Valvular Heart Disease
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease
Practice Questions
Aortic and Great Vessel Imaging
Practice Questions
Peripheral Vascular Imaging
Practice Questions
Cardiovascular Interventional Procedures
Practice Questions
Post-Surgical Cardiovascular Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app