
Cardiovascular Radiology — MCQs

On this page
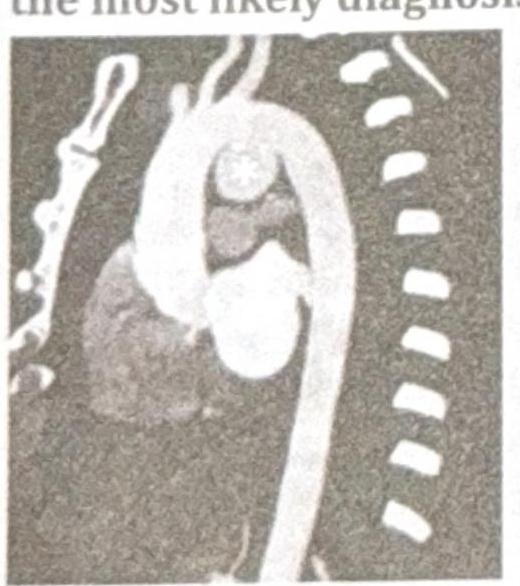
A 38-year-old patient presents with chest pain and hoarseness of voice for the past month. Based on the radiographic image below, what is the most likely diagnosis?
An MRI heart shows 'zebra' pattern in left ventricle. Which additional finding would best support Fabry disease?
An MRA shows 'string of pearls' appearance in renal arteries. Which additional finding would best support fibromuscular dysplasia?
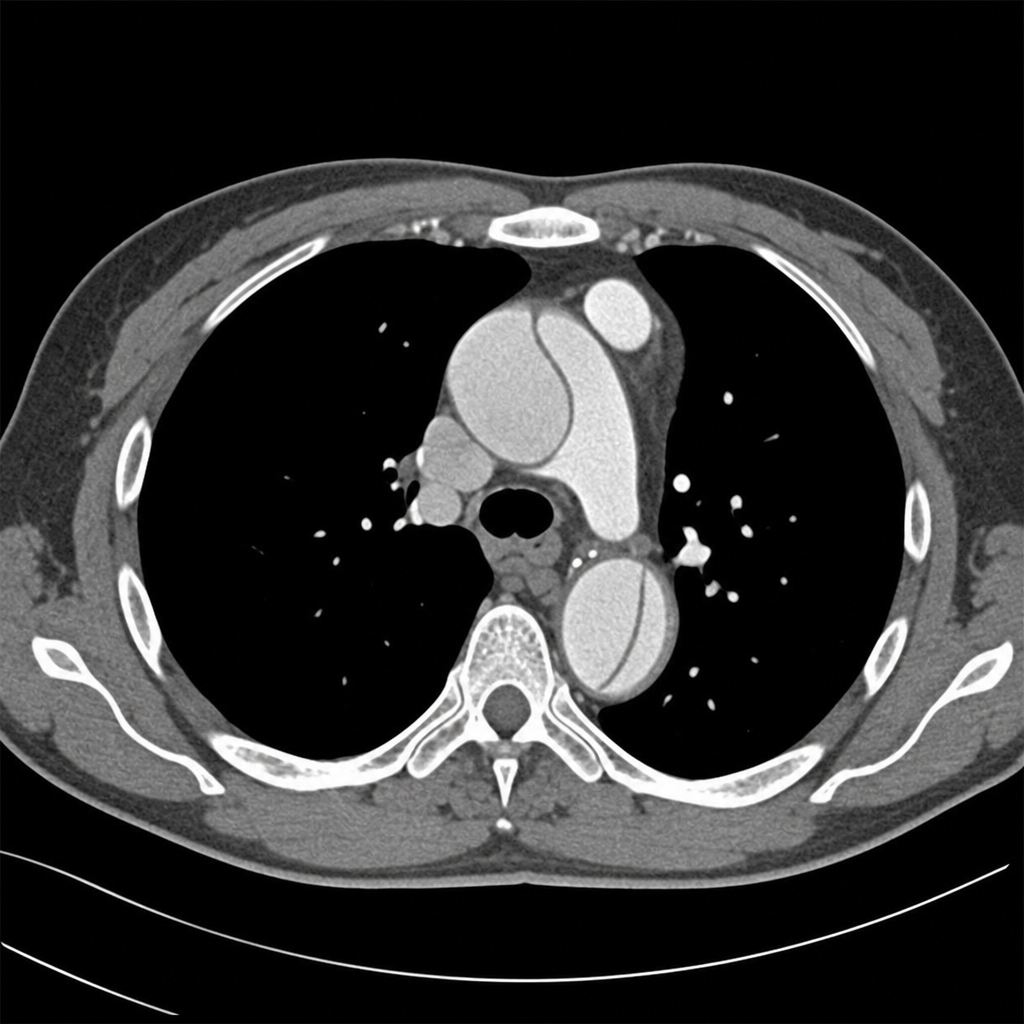
Comment on the diagnosis of the CT chest image shown below.
What is the Investigation of Choice (IOC) for Acute Aortic Dissection?
Pulmonary plethora is not seen in:
In a child with coarctation of aorta, all the following are seen in plain chest radiograph except:
Deep vein thrombosis post-operatively is diagnosed by:
MRI is superior in all of the following conditions except
Aortic calcification is diagnosed on fluoroscopy by identifying:
Practice by Chapter
Cardiovascular Anatomy
Practice Questions
Cardiac CT Techniques
Practice Questions
Cardiac MRI Techniques
Practice Questions
Ischemic Heart Disease Imaging
Practice Questions
Valvular Heart Disease
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease
Practice Questions
Aortic and Great Vessel Imaging
Practice Questions
Peripheral Vascular Imaging
Practice Questions
Cardiovascular Interventional Procedures
Practice Questions
Post-Surgical Cardiovascular Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app