
Congenital Heart Disease — MCQs

A 2-month-old infant is brought to the clinic because of poor feeding, sweating, and difficulty breathing. The parents state that she was doing very well, and has actually been a "very easy going baby", until about a week ago. They assumed that she was developing a "cold", but it has not passed, and the symptoms have been worsening. Cardiac examination reveals a loud, harsh systolic murmur with a thrill that is heard best at the left sternal border. The most likely underlying abnormality is
A 2-week-old girl is found to have a harsh murmur along the left sternal border. The parents report that the baby gets "bluish" when she cries or drinks from her bottle. Echocardiogram reveals a congenital heart defect associated with pulmonary stenosis, ventricular septal defect, dextroposition of the aorta, and right ventricular hypertrophy. What is the appropriate diagnosis?
In a child with coarctation of aorta, all the following are seen in plain chest radiograph except:
A child presented at 10 weeks with recurrent episode of pneumonia and failure to thrive. X-ray shows cardiomegaly & pulmonary plethora. What is the diagnosis?
Which of the following is the most common congenital cardiac malformation?
A 45-year-old woman presents with clubbing and cyanosis. Chest X-ray shows a prominent pulmonary artery. Which congenital heart disease should be considered?
Flask shaped heart is seen in –
Boot shape of heart in TOF is due to:
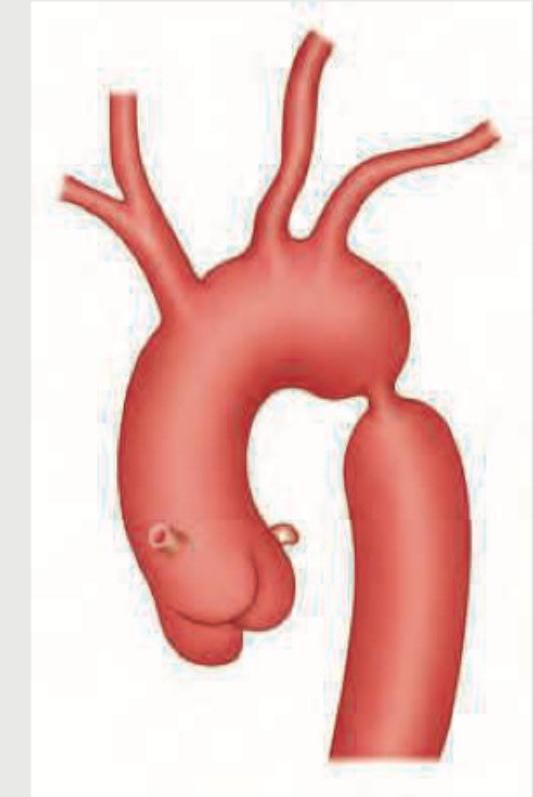
In the condition shown below, rib notching is present in which of the following ribs? (AIIMS Nov 2015)
Radiological features of left ventricular heart failure are all, except -
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app